Diagnosis &Elimination &Ivermectin &MDA &Treatment Bill Brieger | 20 Nov 2016 10:00 am
Leadership and Support for Malaria Pre-Elimination in Nepal
Emmanuel Le Perru, Jhpiego field staff in Nepal, shared his experiences in aiding the malaria pre-elimination efforts in the country during a retreat that preceded the 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. Here are some highlights of his talk.
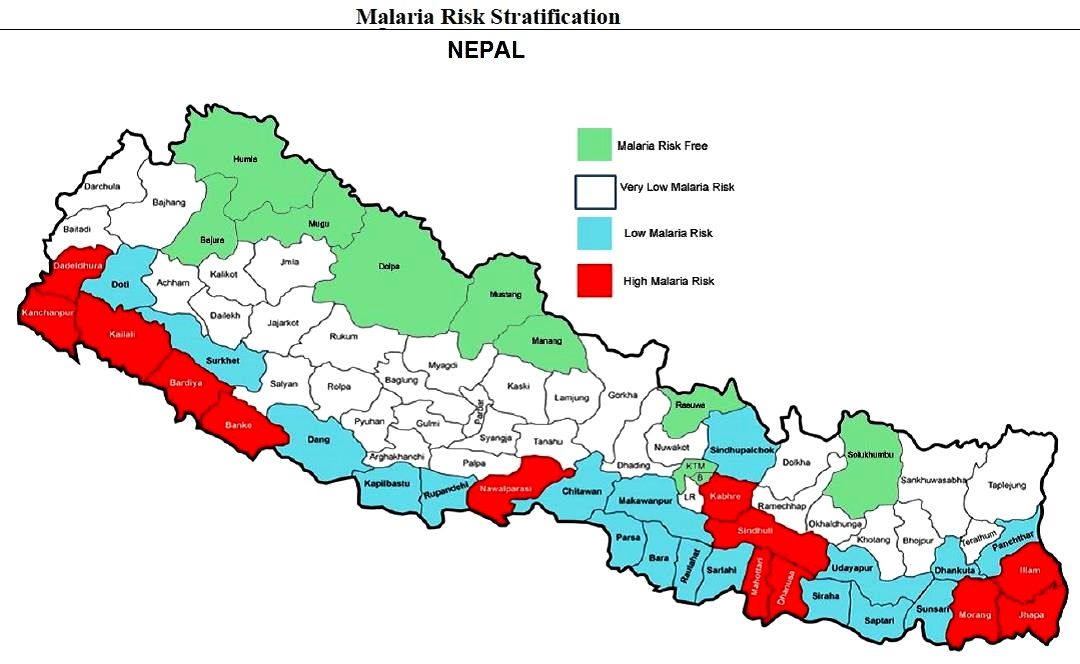 Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Jhpiego is providing technical assistance and capacity building for Nepal’s Ministry of Health pre-elimination efforts as follows:
- Integrated Vector Management
- Micro-stratification
- Entomology curriculum to be conducted in medical college (need new positions)
- Case-based Surveillance guidelines
- Private-sector engagement (for increased reporting and product quality control/procurement such as Antigen RDTs)
- Capacity Assessments in 9 health systems strengthening components at central and district levels (Jhpiego Malaria Implementation Guide)
- Human resources: clear job descriptions and performance goals
- Leadership & Management development program
 Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
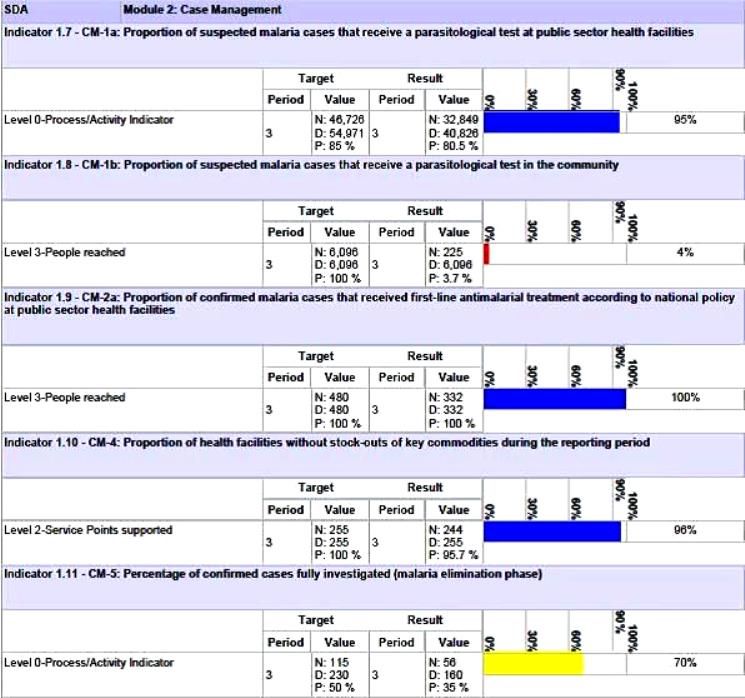
Nepal’s Global Fund Grant Indicators for Malaria Case Management
Although the National Malaria Strategic Plan refers to high risk groups (forest workers, national parks security personnel, refugees, prisoners, etc.) evidence is needed to back this up. A study or improved investigation forms are needed to identify such groups and use this information to design appropriate behavior change communications and other interventions.
Special Programming Highlights include proposing a focus on Closed/Isolated Settings/Foci (limited migration, duration and population) to WHO and GFATM. Considering a targeted mass drug administration (MDA) Plasmodium vivax (not yes recommended by WHO) with Primaquine/G6PD testing. Consideration is being given to new drugs in the pipeline such as Ivermectin. Molecular Testing using Polymerase Chain Reaction (PCR) to detect low parasitemia, asymptomatic or re-infection cases (Pv includes inactive/dormant sporozoites known as hypnozoites) is being proposed.
Community based testing as proposed in the Global Fund grant needs strengthening. Therefore RDT use by Female Community Health Volunteer is being considered. Active case detection is another possibility for those areas moving toward pre-elimination. As mentioned, there is also need for studies of asymptomatic infection.
Lessons learned so far for best practices for efforts in identifying specific pre-elimination interventions include the value of getting consensus at national level through the Malaria Technical Working Group. There is also need to challenge WHO recommendations and engage dialogue to get creative. At present there is a risk of a Catch 22 situation wherein the GFATM asks for innovative interventions but at the same time tries to adhere strictly WHO to existing guidance.
The Nepalese malaria program is in constant dialogue with the GFATM Fund Portfolio Manager and team on the local context and technical challenges in order to get them involved in looking for innovative solutions.
Challenges arise in malaria diagnostics. While systematic microscopy is the gold standard, quality can be poor because of low stain/re-agent quality, constant staff turnover and donor reluctance to fund additional training. Also microscopy confirmation and slide quality control are time consuming, and often this process is not clear or well followed. PCR require specific equipment, training and qualifications. Takes time to be operational.
There are opportunities moving forward. Progress could be made if there were more “elimination experts” to position to influencer to WHO to seek and propose new interventions for the pre-elimination stage. Nepal provides an ideal opportunity to test new ideas. It will also be necessary for the national malaria program staff to receive regular technical updates on program issues such as new drugs (Ivermectin?) and on-going pilots of MDA.