IPTi &Malaria in Pregnancy &Procurement Supply Management Bill Brieger | 15 Nov 2016 07:16 am
Improving IPTp uptake and mitigating Stock-outs in Bungoma County, Kenya
A poster entitled “Improving Pregnancy Outcomes: Alleviating Stock-Outs of Sulfadoxine-Pyrimethamine in Bungoma, Kenya” was presented by Augustine Ngindu, Gathari Ndirangu, Waqo Ejersa, David Omoit, and Mildred Mudany from Jhpiego’s Kenya Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 WHO recommends intermittent preventive treatment of malaria in pregnancy using sulfadoxine pyrimethamine (IPTp-SP) to be provided at antenatal care (ANC) clinic. The Malaria Policy in Kenya requires that All pregnant women in malaria-endemic areas receive free intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), have access to free malaria diagnosis and treatment when presenting with fever, and have access to long-lasting insecticidal nets.
WHO recommends intermittent preventive treatment of malaria in pregnancy using sulfadoxine pyrimethamine (IPTp-SP) to be provided at antenatal care (ANC) clinic. The Malaria Policy in Kenya requires that All pregnant women in malaria-endemic areas receive free intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), have access to free malaria diagnosis and treatment when presenting with fever, and have access to long-lasting insecticidal nets.
Kenya’s Strategic Direction between 2014–2018 was revised to reflect the following:
- All pregnant women in the 14 malaria-endemic counties shall receive at least three doses of IPTp-SP
- Annual quantification of SP based on consumption to ensure adequate supplies
- Training, retraining and supervision of health care workers
- Dissemination of appropriate IPTp messages and materials
 Ministry of Health (MOH) used to procure SP until 2013 when health services were devolved to counties and procurement of became the responsibility of county governments. This presented a major challenge as counties had not factored SP in their budgets. Consequently, counties experienced SP stock-outs from October 2014. In Bungoma County the number of pregnant women receiving IPTp dropped by 51% from 7,845 in October 2014 to 3,865 in February 2015.
Ministry of Health (MOH) used to procure SP until 2013 when health services were devolved to counties and procurement of became the responsibility of county governments. This presented a major challenge as counties had not factored SP in their budgets. Consequently, counties experienced SP stock-outs from October 2014. In Bungoma County the number of pregnant women receiving IPTp dropped by 51% from 7,845 in October 2014 to 3,865 in February 2015.
To alleviate the situation (MOH) at national level requested counties to procure SP. Advocacy efforts with Bungoma County by the Maternal and Child Survival Program focused on prioritization of SP procurement at least once every quarter. As a result of this intervention, Bungoma County procured SP from February to July 2015.
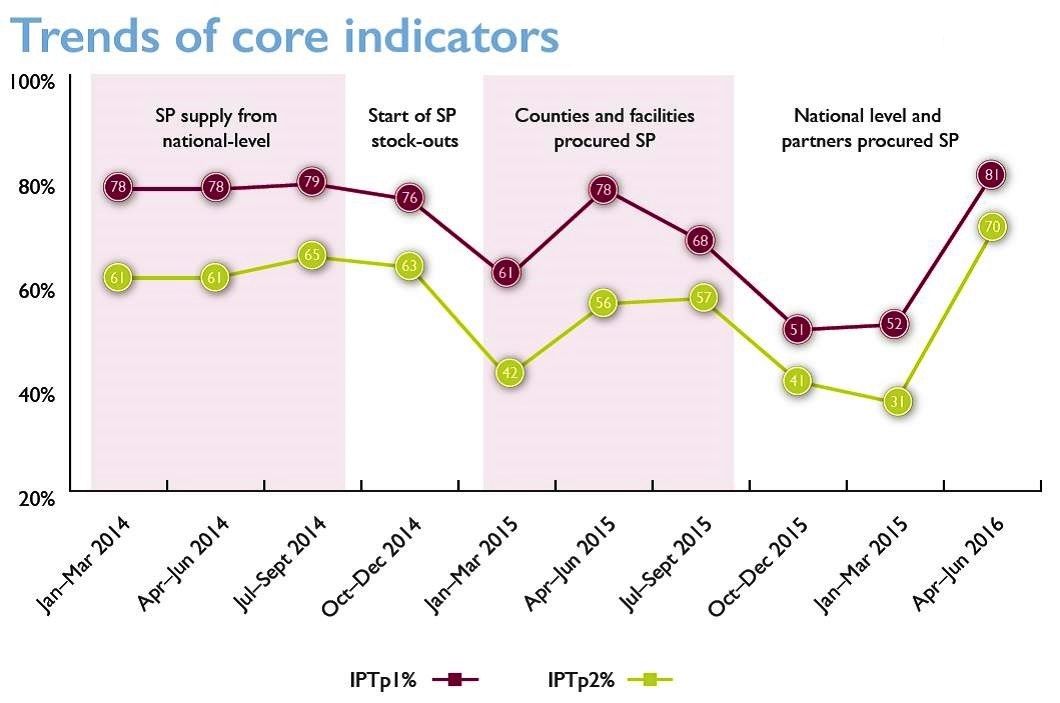 The county advised health facilities to procure additional SP doses if the supplied stocks ran out. The procurement led to a 117% increase in the number of pregnant women receiving IPTp; from 3,865 in February to 8,404 in July 2015.
The county advised health facilities to procure additional SP doses if the supplied stocks ran out. The procurement led to a 117% increase in the number of pregnant women receiving IPTp; from 3,865 in February to 8,404 in July 2015.
The fiscal year ended in June 2015 and no funds were available to procure additional SP until October 2015. This contributed to a 33% decrease in the number of pregnant women receiving IPTp from 8,404 in July to 5,672 in October 2015. As a response to support counties, MOH at national level procured 2.24 million SP doses in November/December for 14 MIP-focus counties which were received at health facilities in February 2016.
In conclusion, Bungoma County applied feasible mitigation measures including county level procurement of SP, supplemented by additional procurement at health facility and national levels. This is a practice which is replicable in other counties to ensure continued availability of SP to protect pregnant women from effects of malaria in pregnancy.