Case Management &Children &Diagnosis &Plasmodium/Parasite Bill Brieger | 23 Nov 2019 04:35 pm
Efficacy of artemether-lumefantrine for the treatment of uncomplicated Plasmodium falciparum infection in Rwanda, 2018
 The Efficacy of artemether-lumefantrine for the treatment of uncomplicated Plasmodium falciparum infection in Rwanda, 2018 was investigated by Aline Uwimana, Noella Umulisa, Eric S. Halsey, Meera Venkatesan, Tharcisse Munyaneza, Rafiki Madjid Habimana, Ryan Sandford, Leah Moriarty, Emily Piercefield, Zhiyong Zhou, Samaly Souza, Naomi Lucchi, Daniel Ngamije, Jean-Louis N Mangala, William Brieger, Venkatachalam Udhayakumar, Aimable Mbituyumuremyi.* The results were presented at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene and are seen below.
The Efficacy of artemether-lumefantrine for the treatment of uncomplicated Plasmodium falciparum infection in Rwanda, 2018 was investigated by Aline Uwimana, Noella Umulisa, Eric S. Halsey, Meera Venkatesan, Tharcisse Munyaneza, Rafiki Madjid Habimana, Ryan Sandford, Leah Moriarty, Emily Piercefield, Zhiyong Zhou, Samaly Souza, Naomi Lucchi, Daniel Ngamije, Jean-Louis N Mangala, William Brieger, Venkatachalam Udhayakumar, Aimable Mbituyumuremyi.* The results were presented at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene and are seen below.
 Background: In Rwanda, there were 4,195,013 confirmed malaria cases and 341 malaria-related deaths in 2018[1]. Regular monitoring of artemisinin-based combination therapy efficacy is important to assess drug efficacy and for timely detection of the emergence of antimalarial drug resistance. In Rwanda, national policy is to routinely monitor the first-line antimalarial per World Health Organization (WHO) guidelines[2] The most recent therapeutic efficacy results in Rwanda showed an efficacy of the first-line antimalarial, artemether-lumefantrine (AL), of >97% in Masaka and Ruhuha in a study conducted from 2013 to 2015[3]
Background: In Rwanda, there were 4,195,013 confirmed malaria cases and 341 malaria-related deaths in 2018[1]. Regular monitoring of artemisinin-based combination therapy efficacy is important to assess drug efficacy and for timely detection of the emergence of antimalarial drug resistance. In Rwanda, national policy is to routinely monitor the first-line antimalarial per World Health Organization (WHO) guidelines[2] The most recent therapeutic efficacy results in Rwanda showed an efficacy of the first-line antimalarial, artemether-lumefantrine (AL), of >97% in Masaka and Ruhuha in a study conducted from 2013 to 2015[3]
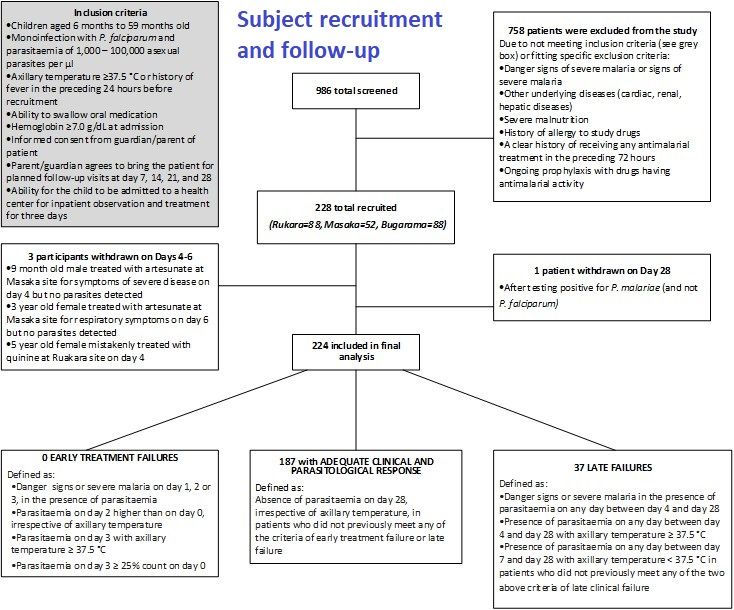
Methods: This was an Efficacy trial based on the standard WHO in vivo protocol[2]. Three sites (see map) were selected in Rwanda. Artemether-lumefantrine (AL) was given twice daily; each dose given under observation for 3 days. Participants were treated with AL and followed for 28 days from March 2018 to December 2018.
 PCR correction, differentiating recrudescence from reinfection in late treatment failure samples, was performed using genotyping of seven neutral microsatellites. Microsatellite data were analyzed using a previously published algorithm that assigns each late treatment failure a posterior probability of recrudescence[4]
PCR correction, differentiating recrudescence from reinfection in late treatment failure samples, was performed using genotyping of seven neutral microsatellites. Microsatellite data were analyzed using a previously published algorithm that assigns each late treatment failure a posterior probability of recrudescence[4]
- Primary Endpoint: 28-day PCR-corrected efficacy
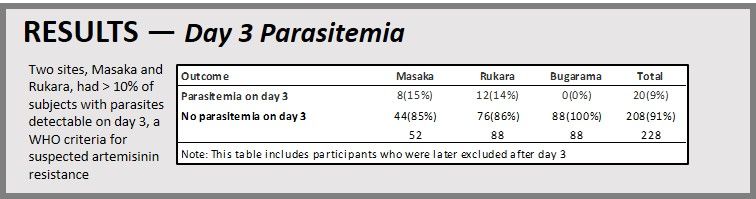
- Secondary Endpoints: 28-day uncorrected efficacy, day 3 parasitemia
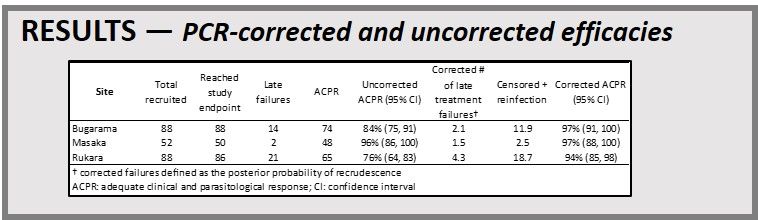 PCR-corrected and uncorrected efficacies are seen to the left. Kaplan Meier Curves are presented. Uncorrected (top) and PCR-corrected (bottom) survival functions for time until failure for a 2018 therapeutic efficacy study using artemether-lumefantrine in three Rwandan study sites; ACPR:
PCR-corrected and uncorrected efficacies are seen to the left. Kaplan Meier Curves are presented. Uncorrected (top) and PCR-corrected (bottom) survival functions for time until failure for a 2018 therapeutic efficacy study using artemether-lumefantrine in three Rwandan study sites; ACPR: 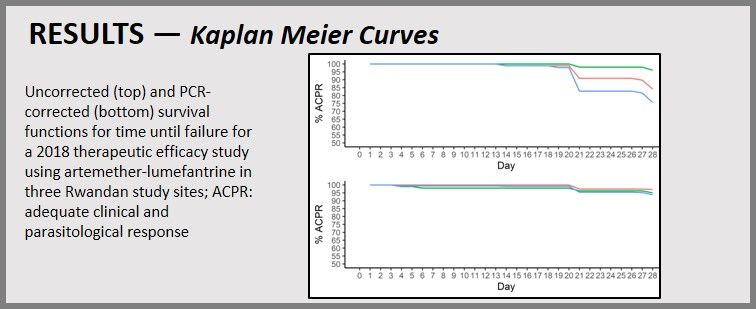 adequate clinical and parasitological response. Day 3 Parasitemia was identified. Two sites, Masaka and Rukara, had > 10% of subjects with parasites detectable on day 3, a WHO criteria for suspected artemisinin resistance.
adequate clinical and parasitological response. Day 3 Parasitemia was identified. Two sites, Masaka and Rukara, had > 10% of subjects with parasites detectable on day 3, a WHO criteria for suspected artemisinin resistance.
 With PCR-corrected efficacies greater than the 90% cut-off recommended by WHO, AL remains an effective antimalarial to treat uncomplicated P. falciparum in Rwanda
With PCR-corrected efficacies greater than the 90% cut-off recommended by WHO, AL remains an effective antimalarial to treat uncomplicated P. falciparum in Rwanda
More than 10% of subjects had day 3 parasitemia at two sites; the relationship with this finding and k13 mutations observed in this study was presented in ASTMH poster LB-5295 (Friday, November 22, 2019).
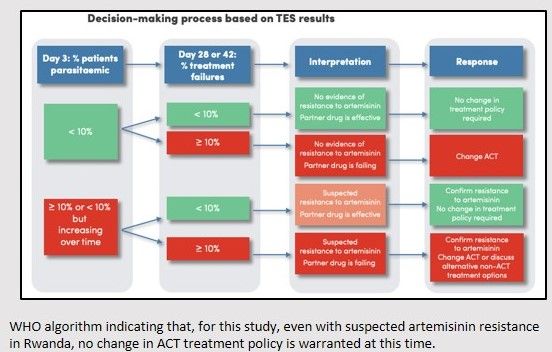 Periodic antimalarial efficacy monitoring in Rwanda should be maintained, and future studies should incorporate additional methods to assess parasite clearance times and presence of molecular markers of resistance. WHO algorithm indicating that, for this study, even with suspected artemisinin resistance in Rwanda, no change in ACT treatment policy is warranted at this time.
Periodic antimalarial efficacy monitoring in Rwanda should be maintained, and future studies should incorporate additional methods to assess parasite clearance times and presence of molecular markers of resistance. WHO algorithm indicating that, for this study, even with suspected artemisinin resistance in Rwanda, no change in ACT treatment policy is warranted at this time.
References
- Rwanda Malaria and Other Parasitic Diseases Division, Rwanda Biomedical Center, HMIS data, 2018.
- WHO, Methods for Surveillance of Antimalarial Drug Efficacy, 2009.
- Uwimana A, Efficacy of artemether–lumefantrine versus dihydroartemisinin–piperaquine for the treatment of uncomplicated malaria among children in Rwanda: an open-label, randomized controlled trial, Trans R Soc Trop Med Hyg; doi:10.1093/trstmh/trz009; 2019.
- Plucinski MM, Morton L, Bushman M, Dimbu PR, Udhayakumar V. Robust algorithm for systematic classification of malaria late treatment failures as recrudescence or reinfection using microsatellite genotyping. Antimicrob Agents Chemother;59:6096–100; 2015.
Contact Information: Aline Uwimana, MD: aline.uwimana@rbc.gov.rw and Eric Halsey, MD: ycw8@cdc.gov
*Affiliations: Malaria and Other Parasitic Diseases Division, Rwanda Biomedical Centre, Kigali, Rwanda; Maternal and Child Survival Program/JHPIEGO, Baltimore MD, USA; The US President’s Malaria Initiative, Atlanta, Georgia, USA; Malaria Branch, Centers for Disease Control and Prevention, Atlanta, Georgia, USA; US President’s Malaria Initiative, Washington DC, USA; National Reference Laboratory, Rwanda Biomedical Centre, Kigali, Rwanda; US Peace Corps, Kigali, Rwanda; US President’s Malaria Initiative, Kigali, Rwanda; WHO Rwanda Office, Malaria and Neglected Tropical Diseases Programs, Kigali, Rwanda; The Johns Hopkins University, Bloomberg School of Public Health, Department of International Health, Baltimore, MD, USA