Advocacy &IPTi &Malaria in Pregnancy Bill Brieger | 16 Nov 2016 07:03 am
Country Updates on Global Call to Action to Increase Coverage of Intermittent Preventive Treatment in Pregnancy
Symposium 87 at the 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene focused on the Global Call to Action to Increase Coverage of Intermittent Preventive Treatment in Pregnancy: Progress and Lessons Learned. The original Global Call was initiated at a previous ASTMH meeting. Elaine Roman of Jhpiego chaired the session. Panelists included Julie Gutman of the US CDC, Frank Chacky of the NMCP in Tanzania, Yacouba Savadogo of the NMCP in Burkina Faso and Fannie Kachale of the Reproductive Health Directorate in the Malawi MOH.
 The symposium speakers reviewed country progress in sub-Saharan Africa (SSA) in increasing intermittent preventative treatment in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP). They described how Ministries of Health and donors and partners are working to increase IPTp-SP coverage to address malaria in pregnancy (MiP).
The symposium speakers reviewed country progress in sub-Saharan Africa (SSA) in increasing intermittent preventative treatment in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP). They described how Ministries of Health and donors and partners are working to increase IPTp-SP coverage to address malaria in pregnancy (MiP).
Following the release of the World Health Organization’s (WHO) 2012 updated policy on IPTp-SP, a number of global stakeholders came together through the Roll Back Malaria-Malaria in Pregnancy Working Group, to elaborate the Global Call to Action: To Increase National Coverage with IPTp of MiP for Immediate Impact. The Call to Action calls upon countries and partners to immediately scale up IPTp-SP to improve health outcomes for mothers and their newborns. Scaling up IPTp-SP across most countries in sub-Saharan Africa remains a critical weapon to prevent the devastating consequences of MiP.
IPTp3+ has been started in Malawi following WHO recommendations
However, the low proportion of eligible pregnant women receiving at least one dose of IPTp-SP (52%) and IPTp3-SP (17%) in 2014 is unacceptable. Despite growing parasite resistance to SP in some areas, IPTp-SP remains Tuesday a highly cost-effective, life-saving strategy to prevent the adverse effects of MiP in the vast majority of SSA.
Completion of the recommended three or more doses of IPTp-SP decreases the incidence of low birthweight (LBW) by 27%, severe maternal anemia by 40% and neonatal mortality by 38%. This symposium will feature presentations from WHO and the President’s Malaria Initiative on how they are prioritizing support to scale up MiP interventions including IPTp-SP across SSA.
Panelists from Burkina Faso, Malawi and Tanzania discussed how they were able to dramatically scale up IPTp-SP through a health systems approach that addresses MiP from community to district to national level.
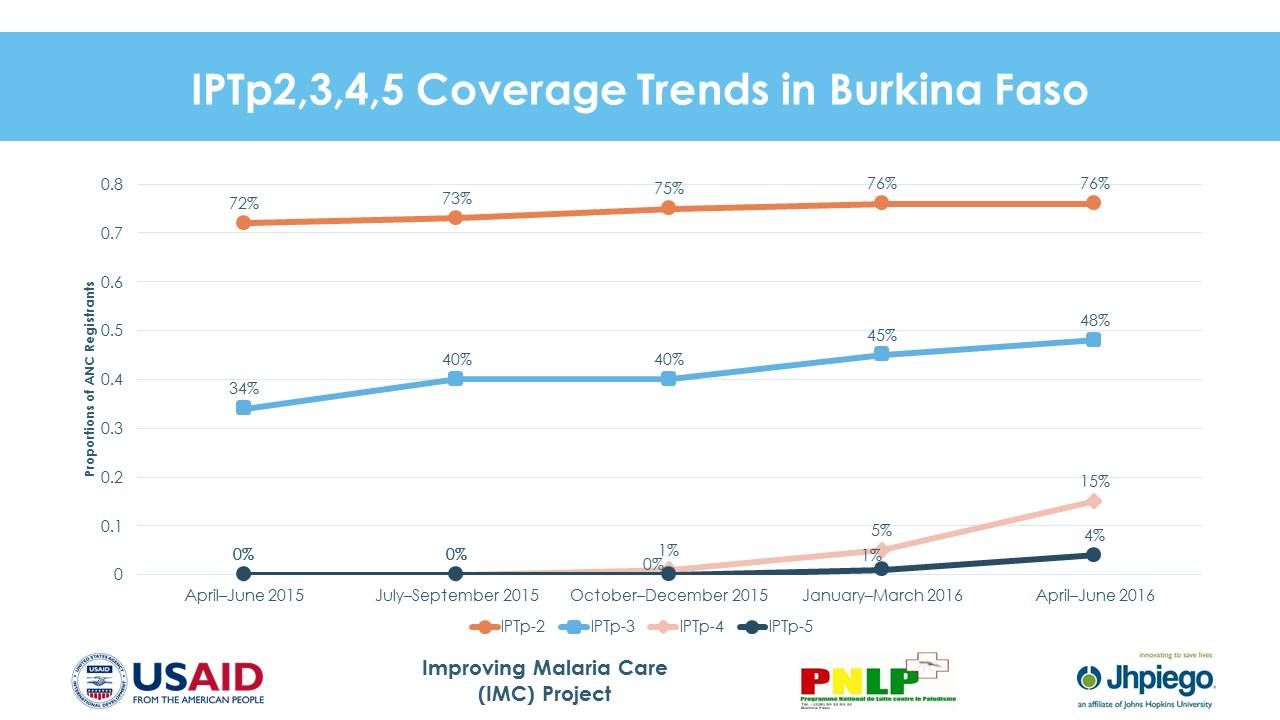 In Burkina Faso, IPTp2-SP increased from 54.8% in 2013 to 82.3% nationally in 2015 and IPTp3-SP increased from 13.5% in 2014 to 41.2% nationally in 2015. Moving ahead Burkina Faso will Improve SP supply chain management, Pilot an IPTp distribution at the community level in three districts, Provide job aids throughout ANC clinics, and Provide support to district team for data review and analysis.
In Burkina Faso, IPTp2-SP increased from 54.8% in 2013 to 82.3% nationally in 2015 and IPTp3-SP increased from 13.5% in 2014 to 41.2% nationally in 2015. Moving ahead Burkina Faso will Improve SP supply chain management, Pilot an IPTp distribution at the community level in three districts, Provide job aids throughout ANC clinics, and Provide support to district team for data review and analysis.
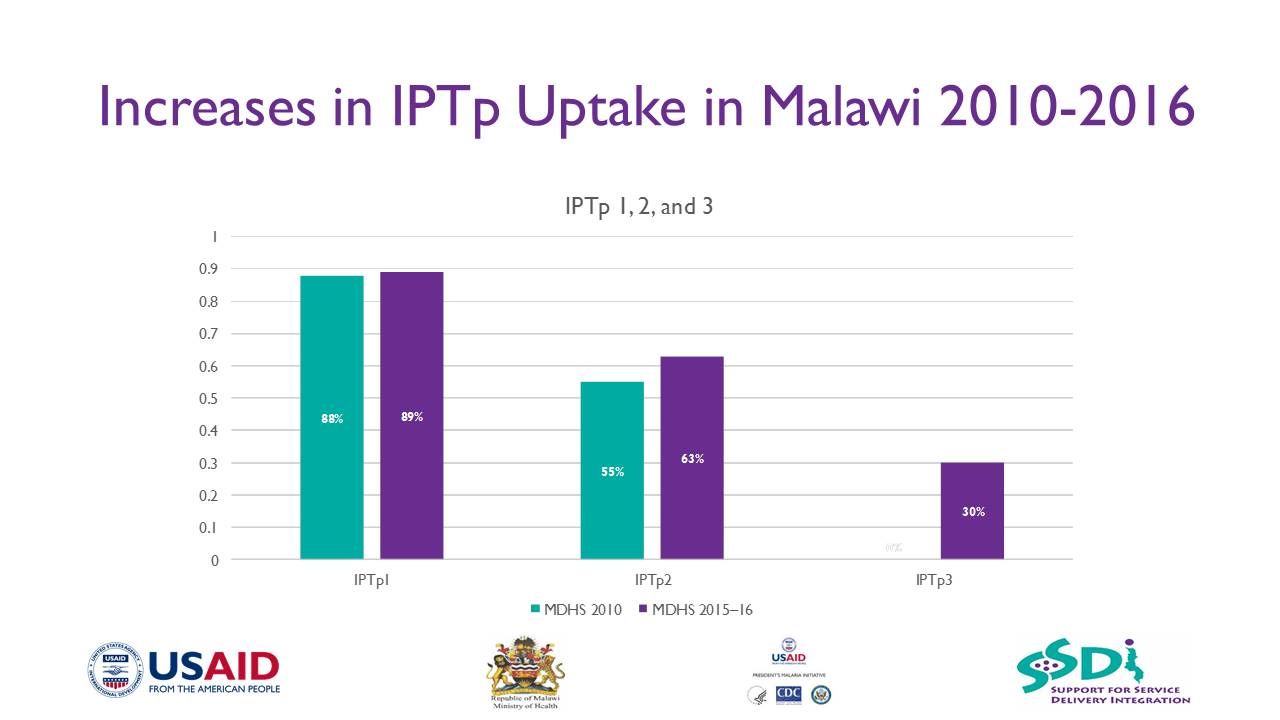
In Malawi, in targeted project sites across 15 districts, IPTp1 uptake increased from 44% in 2012 to 87% in 2015, while IPT2 increased from 16% to 61% over the same time period. Lessons learned from scale up include –
- Consistent availability of SP for IPTp is critical to increasing coverage
- A clear policy put in place to guide IPTp implementation is crucial

- A strong partnership between the Reproductive Health Directorate and National Malaria Control Programme is necessary
- Intensification of information, education, and communication is crucial to increase uptake of ANC services
- Strong collaboration, planning, and coordination between partners and other stakeholders improve ANC attendance
- Antenatal clinics offers enormous opportunities for delivering the malaria prevention package, such as IPTp and insecticide-treated nets, to pregnant women
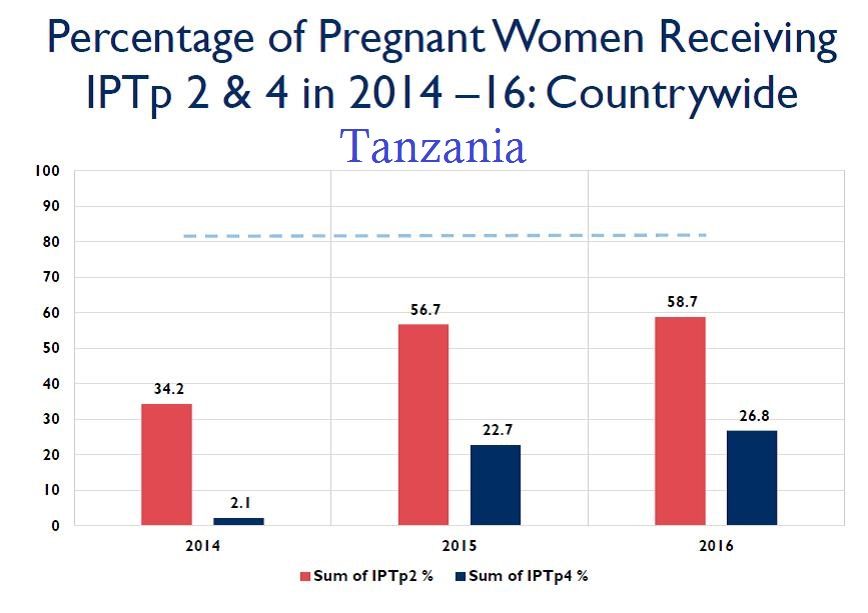 In Tanzania, IPTp2-SP increased from 34% in 2014 to 57% in 2015 and IPTp4-SP was reported at 22% in 225 facilities across 16 districts, in 2015. Program learning in Tanzania identified that consistent availability of commodities at facility level can complement Government’s and partners’ efforts to ensure provision of quality MiP services. Despite increased number of trained health care workers and regular supportive supervision and mentoring, increasing uptake of IPTp will continue to be a challenge unless malaria commodities such as mRDT and SP are available at health facilities. Redistribution of commodities among facilities could be crucial balancing the stock.
In Tanzania, IPTp2-SP increased from 34% in 2014 to 57% in 2015 and IPTp4-SP was reported at 22% in 225 facilities across 16 districts, in 2015. Program learning in Tanzania identified that consistent availability of commodities at facility level can complement Government’s and partners’ efforts to ensure provision of quality MiP services. Despite increased number of trained health care workers and regular supportive supervision and mentoring, increasing uptake of IPTp will continue to be a challenge unless malaria commodities such as mRDT and SP are available at health facilities. Redistribution of commodities among facilities could be crucial balancing the stock.
 Moving forward Tanzania plans to use alternative funding to procure malaria commodities at health facility (e.g., Community Health Fund, National Health Insurance Fund, basket fund). Other efforts will include conducting onsite mentorship and coaching, data collection and interpretation, selecting sentinel sites for collecting IPTp3, working with Ministry of Health HMIS to revise HMIS tools when opportunity arises, and training Community Health Workers (CHWs) on maternal, neonatal and child health interventions including early booking of ANC services.
Moving forward Tanzania plans to use alternative funding to procure malaria commodities at health facility (e.g., Community Health Fund, National Health Insurance Fund, basket fund). Other efforts will include conducting onsite mentorship and coaching, data collection and interpretation, selecting sentinel sites for collecting IPTp3, working with Ministry of Health HMIS to revise HMIS tools when opportunity arises, and training Community Health Workers (CHWs) on maternal, neonatal and child health interventions including early booking of ANC services.
These three country examples demonstrate that progress is challenging but possible. The call to action for increased IPTp access and use is stronger today.