Invest in Malaria Control &IRS &Malaria in Pregnancy Bill Brieger | 15 Apr 2015
Investing in Antenatal Care to Defeat Malaria
For many years malaria in pregnancy (MIP) was the proverbial neglected step-child of malaria control programs. Partly this was due to structural problems – the challenge of coordination between different units and departments within a ministry of health – malaria programs and reproductive health programs in separate and parallel divisions.
Another reason for neglect may lie in the fact that it is been difficult to achieve the MDG 5 as outlined in the United Nations’ 2014 Millennium Development Goals Report. One still finds that worldwide, almost 300,000 women died in 2013 from causes related to pregnancy and childbirth. Maternal death is mostly preventable and much more needs to be done to provide care to pregnant women.
Maternal death prevention includes providing pregnant women 3 or more doses of sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment in pregnancy (IPTp) and ensuring women have AND sleep under insecticide treated bednets (ITNs) during antenatal care (ANC). Unfortunately recent Demographic and Health Surveys (DHS) and Malaria Information Surveys (MIS) from endemic countries show slow or stagnating progress in reaching Roll Back Malaria goals of 80% coverage of pregnant women with these interventions. Recent DHS/MIS have found that only 15% of recently pregnant women got two doses of IPTp in Nigeria, with only slightly better coverage in Burkina Faso (46%). Now that targets have shifted to three or more doses, the coverage challenge is even greater.
 The irony is that these same DHS reports show that a large proportion (>90%) of pregnant women in malaria endemic countries of Africa get registered for ANC. In order to achieve full coverage of IPTp pregnant women should attend ANC at least four times, but the recommended minimum of four ANC visits is difficult to achieve. According to WHO, “The proportion of pregnant women in developing countries who attended at least four antenatal care visit has increased from approximately 37% in 1990 to about 52% in 2012 but, in low-income countries, only 38% of pregnant women attended four times or more antenatal care during 2006-2013.”
The irony is that these same DHS reports show that a large proportion (>90%) of pregnant women in malaria endemic countries of Africa get registered for ANC. In order to achieve full coverage of IPTp pregnant women should attend ANC at least four times, but the recommended minimum of four ANC visits is difficult to achieve. According to WHO, “The proportion of pregnant women in developing countries who attended at least four antenatal care visit has increased from approximately 37% in 1990 to about 52% in 2012 but, in low-income countries, only 38% of pregnant women attended four times or more antenatal care during 2006-2013.”
In their article, “The quality–coverage gap in antenatal care: toward better measurement of effective coverage,” Stephen Hodgins and Alexis D’Agostino offer an explanation. They point out that it is not the number of ANC contacts alone that matters; it is the content of each visit that is equally important. They explain that a “coverage gap” exists when women who attended ANC four or more times did not receive the elements of basic package of services spelled out in the concept of Focused Antenatal Care (FANC).
Specific findings from Hodgins and D’Agostino’s DHS review showed that, “Blood pressure and tetanus toxoid performed best, with median quality–coverage gaps of 5% and 18%, respectively. The greatest gaps were for iron–folate supplementation (72%) and malaria prevention (86%).” Simply put, the lesson is that attending ANC does not equal receiving lifesaving maternal health services.
Many factors affect the quality of ANC services ranging from the major gaps in availability of trained health workers at the frontline in endemic countries to poor procurement and supply systems for even the cheapest drugs like SP. Even when health workers are in place, their understanding of and attitudes toward using SP for IPTp may be inadequate. These issues are where the gap between attending ANC and receiving needed services emerges. We will not be able to defeat malaria in pregnancy until we invest in strengthening the whole ANC system and pay better attention of women’s health.
Invest in Malaria Control &ITNs Bill Brieger | 09 Apr 2015
Monitoring Net Use: Ensuring a Major Investment Pays Off
 John Orok, the Director of Akwa Ibom State’s Malaria Control Program in Nigeria, and colleagues have shared with us the follow-up survey results following a mass LLIN distribution campaign in his state in late 2014. Unless we monitor our investments in nets, we will not “Defeat Malaria.”
John Orok, the Director of Akwa Ibom State’s Malaria Control Program in Nigeria, and colleagues have shared with us the follow-up survey results following a mass LLIN distribution campaign in his state in late 2014. Unless we monitor our investments in nets, we will not “Defeat Malaria.”
While long lasting insecticide-treated nets (LLINs) have made a major dent in the incidence of malaria in Africa, LLINs need to be replaced at intervals. Akwa Ibom State Ministry of Health (SMOH) conducted a mass net distribution in 2010 during which 1.8 million LLINs were handed out in the 31  local government areas (LGAs/Districts). An estimated 2.7 million nets were acquired with Global Fund support for replacement distribution in November and December 2014. In an effort to learn about the outcome of the exercise, the SMOH organized a follow-up household survey in all LGAs in January 2015.
local government areas (LGAs/Districts). An estimated 2.7 million nets were acquired with Global Fund support for replacement distribution in November and December 2014. In an effort to learn about the outcome of the exercise, the SMOH organized a follow-up household survey in all LGAs in January 2015.
The state formed a technical working group which developed a checklist and interview guide for to gather follow-up information on the number of households that acquired nets, hung the nets, slept under the nets, their reasons for not using nets and sources of information about nets. Interviewers were recruited for each LGA and trained to use the checklist and recognize appropriate net hanging and use. Twelve interviewers were assigned to each Ward of each LGA.
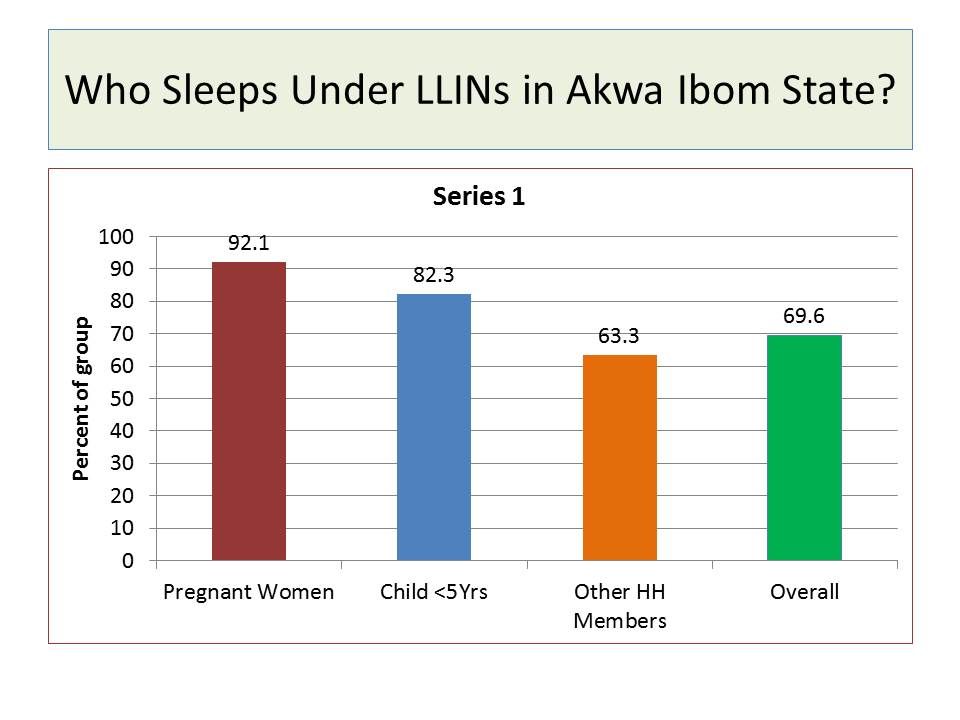 A total of 2,696,476 net cards were issued to households based on approximately two nets per household, and 2,626,966 nets (97.4%) were redeemed. Retention rate in the sampled households was 97.1%, while hanging rate of those retained was 71.8%%. Overall 69.6% household members reported that they slept under a net the previous night. A greater proportion of pregnant women (92.1%) reported using nets compared to children below 5 years of age (82.3%) and other household members (63.3%). Main reasons for not using nets included feeling hot (44.5%), inability to hang the net (19.7%) and concern about the chemical used to treat the net (11.4%).
A total of 2,696,476 net cards were issued to households based on approximately two nets per household, and 2,626,966 nets (97.4%) were redeemed. Retention rate in the sampled households was 97.1%, while hanging rate of those retained was 71.8%%. Overall 69.6% household members reported that they slept under a net the previous night. A greater proportion of pregnant women (92.1%) reported using nets compared to children below 5 years of age (82.3%) and other household members (63.3%). Main reasons for not using nets included feeling hot (44.5%), inability to hang the net (19.7%) and concern about the chemical used to treat the net (11.4%).
Akwa Ibom is located in Nigeria’s highest malaria transmission zone, and hence there is need to use LLINs throughout the year. The contrast with 2013 DHS, where only 14.1% of residents overall slept under an LLIN, results is stark and implies that net use may likely decline as nets age beyond an ideal replacement schedule of every 2-3 years. Even 1-2 months out from a campaign there are people who are not hanging and using nets. Continuous systems for community level education and reinforcement and health system-based routine distribution for periods between campaigns are needed to ensure this major investment in controlling malaria pays off..