CHW &Community &Equity &Health Workers &ITNs Bill Brieger | 12 Mar 2018
Malaria by the numbers: are the statistics real or are they a barrier to community involvement?
 George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
——-
 I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
Today malaria is still among the top causes of infant mortality in many African countries, including Ghana, yet we have mosquito nets, coils, sprays, long sleeved shirts that have been circulating in the country for years……and sometimes I wonder: why?
Total funding for malaria prevention and control was 2.7 billion dollars in 2016. Between 2014-2016, 582 million nets were distributed, of which 505 million were distributed in Africa, yet the number of malaria cases increased from 211 million in 2015 to 216 million in 2016 (WHO-malaria fact sheet, 2017).
I was once a supervisor for the distribution of long-lasting insecticide treated nets in rural communities. The numbers driven world saw big numbers that showed that many pregnant women were not sleeping under mosquito nets and so the solution to solve the malaria problem was to give them mosquito nets.
 First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
This time we went into a house with a hammer, nails and ropes, and families showed us their bedroom and we hung the net for them. And yet malaria still rules. What happened with the free bed nets is now widely reported across different countries in Africa.
What do the numbers we measure mean to the people they represent?
 As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
Frustrations abound on both ends of the system, for public health agents and community members. Numbers act as the barrier between the two ends of the “system”, and our goal must be to break the barrier. The numbers that drive interventions can be meaningless to the community people they represent unless we engage the community and learn how our interventions can really help them.
Health Workers &IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2017
Improving intermittent preventive treatment for pregnant women (IPTp) coverage in 5 districts in Chad and Cameroon
 Kodjo Morgah and Naibei Mbaïbardoum of Jhpiego with support from the ExxonMobil Foundation ave been working to increase interventions that protect pregnant women from malaria. The results below were shared at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Kodjo Morgah and Naibei Mbaïbardoum of Jhpiego with support from the ExxonMobil Foundation ave been working to increase interventions that protect pregnant women from malaria. The results below were shared at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Malaria is the leading cause of morbidity and mortality in Cameroon and Chad, where an estimated 500,000 and 1.5 million cases occur every year, respectively. In Cameroon, 55% of hospitalizations and 241 deaths among pregnant women reported in 2010 were due to malaria. In Chad, malaria accounted for 30% of hospital admissions and 41% of deaths among pregnant women in 2013.
 To improve uptake of intermittent preventive treatment for pregnant women (IPTp) for malaria in 5 districts in Chad and the Kribi district of Cameroon, Jhpiego adopted strategies targeting the 4 levels of the health system in each country: updating national policies and guidelines, building capacity of providers, building community health workers’ (CHWs) capacity, and engaging in behavior change communication.
To improve uptake of intermittent preventive treatment for pregnant women (IPTp) for malaria in 5 districts in Chad and the Kribi district of Cameroon, Jhpiego adopted strategies targeting the 4 levels of the health system in each country: updating national policies and guidelines, building capacity of providers, building community health workers’ (CHWs) capacity, and engaging in behavior change communication.
 Nationally, Jhpiego provided technical guidance to the Ministries of Health to develop tools including: training and malaria in pregnancy (MIP) reference manuals for providers and CHWs, guidelines on IPTp, and key supervision and data collection tools. At the regional/district levels, 38 supervisors were trained, and they conducted 248 supervisory visits in both countries, reaching 137 health facilities.
Nationally, Jhpiego provided technical guidance to the Ministries of Health to develop tools including: training and malaria in pregnancy (MIP) reference manuals for providers and CHWs, guidelines on IPTp, and key supervision and data collection tools. At the regional/district levels, 38 supervisors were trained, and they conducted 248 supervisory visits in both countries, reaching 137 health facilities.
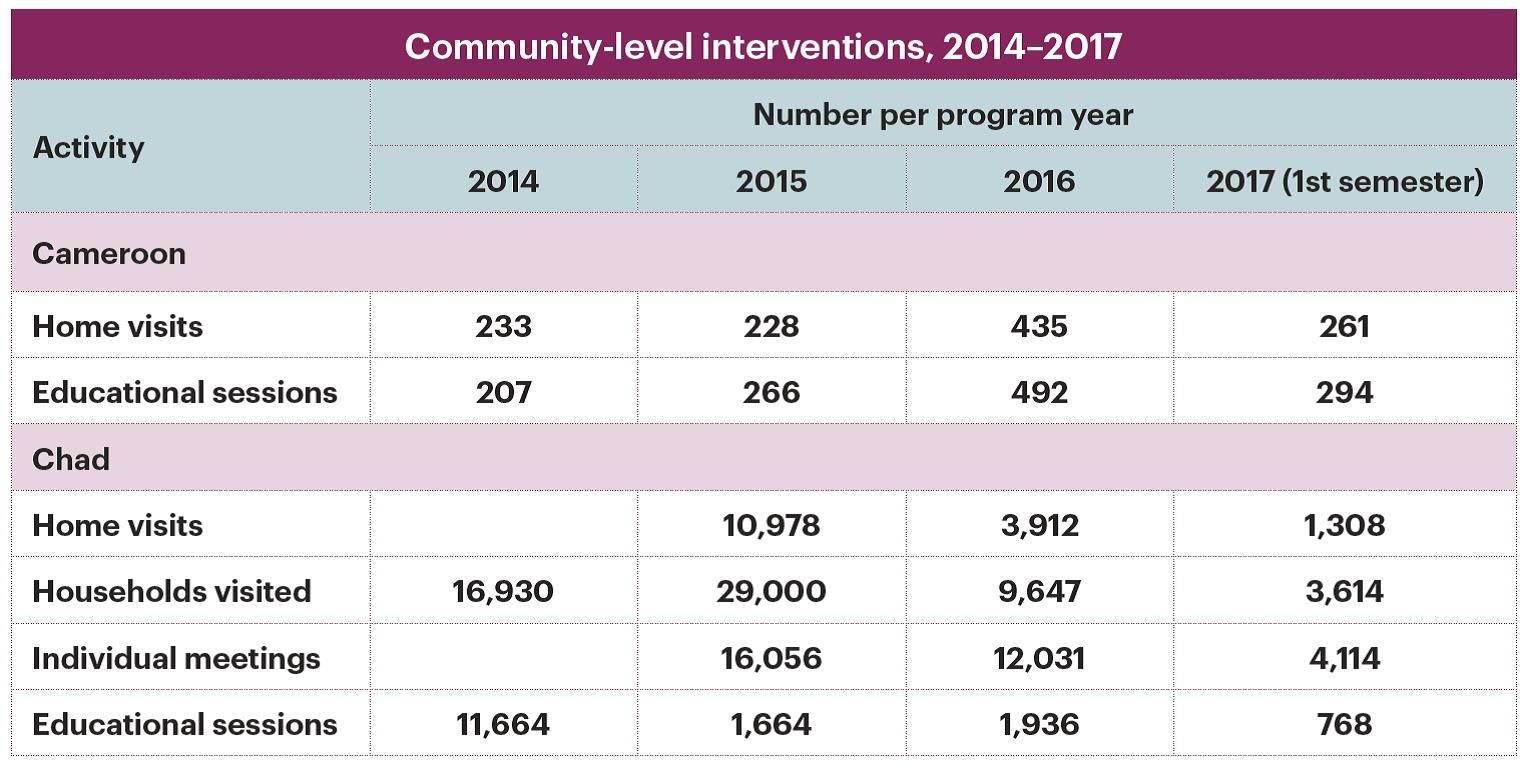
 At the facility level, 234 providers were trained in malaria prevention and management, MIP, data collection and commodity management. At the community level, 146 CHWs in both countries were trained to raise awareness on malaria prevention and control.
At the facility level, 234 providers were trained in malaria prevention and management, MIP, data collection and commodity management. At the community level, 146 CHWs in both countries were trained to raise awareness on malaria prevention and control.
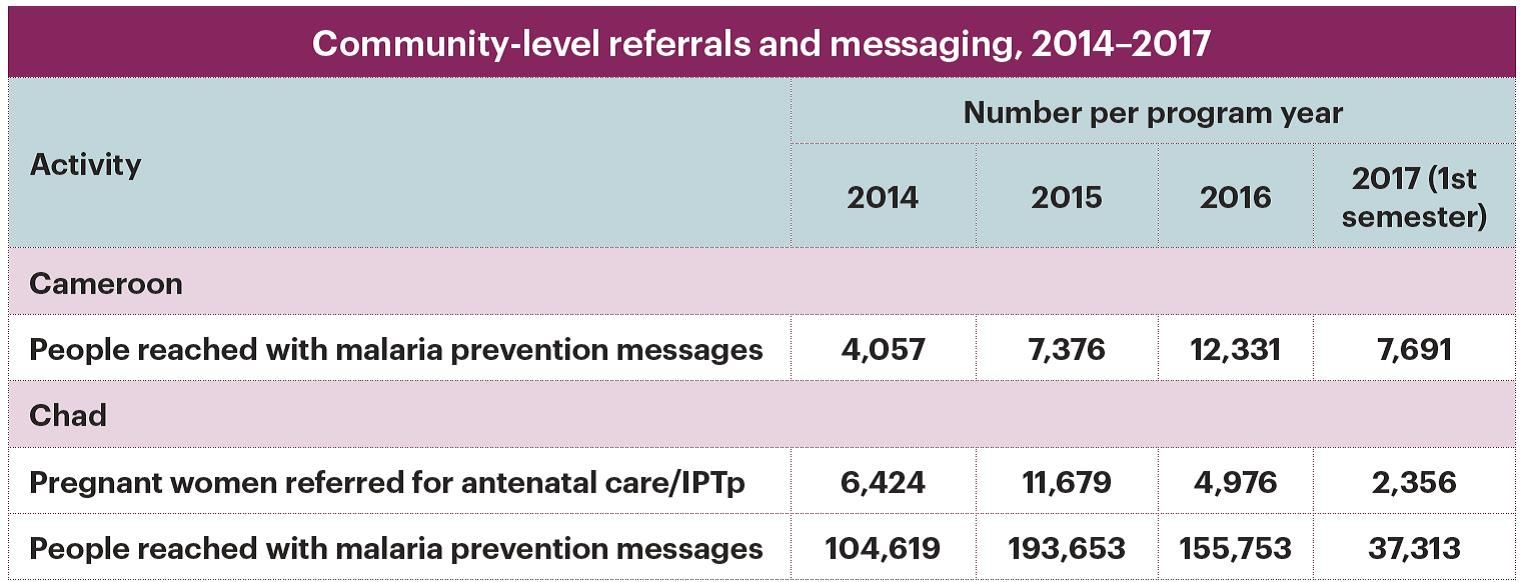
 In Chad, CHWs referred 6424 pregnant women for antenatal care/IPTp and 11679 pregnant women for malaria treatment in 2014 and 2015. Health facility and CHW data collection tools were revised and monthly validation of district data was implemented to improve data reliability, completeness, and readiness.
In Chad, CHWs referred 6424 pregnant women for antenatal care/IPTp and 11679 pregnant women for malaria treatment in 2014 and 2015. Health facility and CHW data collection tools were revised and monthly validation of district data was implemented to improve data reliability, completeness, and readiness.
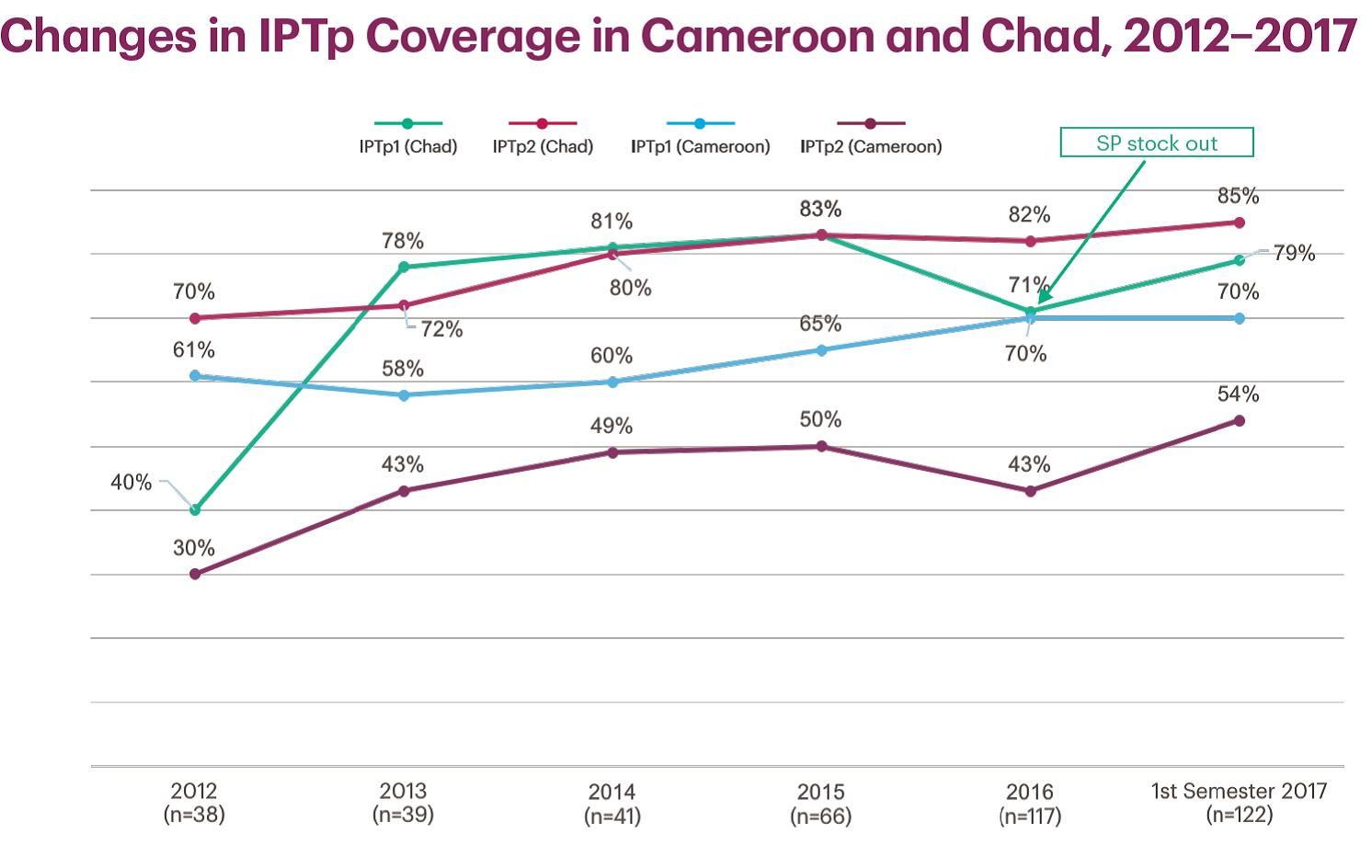
As a result of Jhpiego’s activities in Kribi, IPTp rates increased from the start of the project in 2012 to 2015: from 70% to 83% (IPTp1), 61% to 80% (IPTp2), and 12.7% to 28.1% (IPTp3). Similarly, from 2012 to 2015 in Chad, IPTp1 rates increased from 40% to 83% and from 30% to 50% for IPTp2. These gains are a result of training paired with coaching and supervision activities of trained providers and targeted facilities.
Health Workers &IPTp &Malaria in Pregnancy &Performance &Quality of Services Bill Brieger | 09 Nov 2017
Results of an evaluation of the Toolkit to Improve Early and Sustained Intermittent Preventive Treatment in Pregnancy (IPTp) Uptake in Mozambique and Madagascar
 Lalanirina Ravony, Elana Fiekowsky, Lisa Noguchi, Patricia P. Gomez, Jean Pierre Rakotovao, Eliane Razafimandimby, Armindo Tiago, Kathryn Smock, Arsene Ratsimbarisoa, Kristen Vibbert, and Robert Sellke shared their efforts to apply a toolkit to enable health providers to ensure better uptake of intermittent preventive treatment for malaria during antenatal clinics. As seen below, they presented their findings at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Lalanirina Ravony, Elana Fiekowsky, Lisa Noguchi, Patricia P. Gomez, Jean Pierre Rakotovao, Eliane Razafimandimby, Armindo Tiago, Kathryn Smock, Arsene Ratsimbarisoa, Kristen Vibbert, and Robert Sellke shared their efforts to apply a toolkit to enable health providers to ensure better uptake of intermittent preventive treatment for malaria during antenatal clinics. As seen below, they presented their findings at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
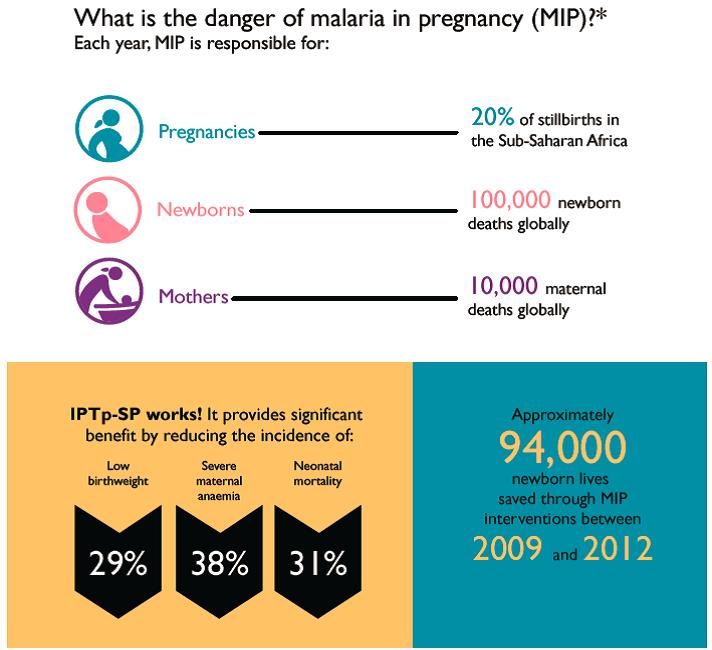
Malaria in pregnancy (MIP) is a leading cause of maternal and newborn morbidity and mortality; however uptake of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP), an effective prevention tool, remains alarmingly low across sub-Saharan Africa, including Mozambique and Madagascar.
 The WHO 2012 policy recommendations to prevent MIP include early enrollment into antenatal care (ANC), accurate estimation of gestational age (GA) and administration of IPTp-SP during ANC visits beginning early in the second trimester, spaced at least one month apart. Preventing MIP remains a challenge in settings with inconsistent application of these recommendations and inadequate provider training in estimating GA.
The WHO 2012 policy recommendations to prevent MIP include early enrollment into antenatal care (ANC), accurate estimation of gestational age (GA) and administration of IPTp-SP during ANC visits beginning early in the second trimester, spaced at least one month apart. Preventing MIP remains a challenge in settings with inconsistent application of these recommendations and inadequate provider training in estimating GA.
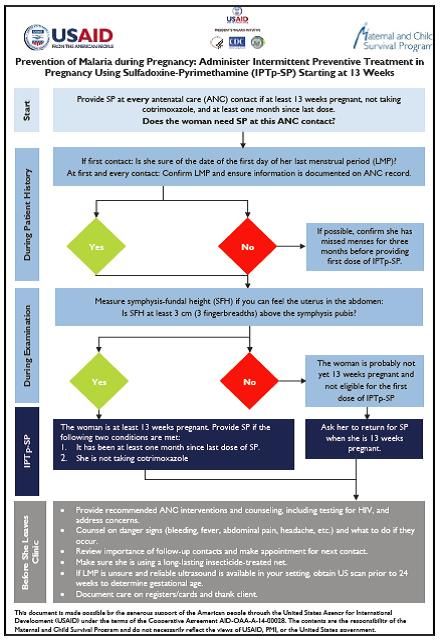 To improve adherence to these recommendations, a toolkit was designed which includes a job aid with an algorithm to guide providers during ANC visits to determine IPTp-SP eligibility. Twenty-four providers from 24 facilities in Madagascar and 29 providers from seven facilities in Mozambique were trained on use of the job aid and interviewed three months later about their experience.
To improve adherence to these recommendations, a toolkit was designed which includes a job aid with an algorithm to guide providers during ANC visits to determine IPTp-SP eligibility. Twenty-four providers from 24 facilities in Madagascar and 29 providers from seven facilities in Mozambique were trained on use of the job aid and interviewed three months later about their experience.
Individual providers were interviewed using a questionnaire to assess the clarity and utility to the job aid, and their opinions of the practicality of the orientation. Interviewers also gathered information on years of experience and clinical certification. All providers reported that the job aid reminded them to estimate GA and measure fundal height, which is particularly helpful since few women remember the date of their last menstrual period (LMP).
 Health workers also reported that the job helped them encourage the use of long-lasted insecticide treated nets, and reminded them of the proper timing to start IPTp-SP. We conclude that the toolkit is useful to prompt providers to calculate GA and offer IPTp as early as possible in the second trimester.
Health workers also reported that the job helped them encourage the use of long-lasted insecticide treated nets, and reminded them of the proper timing to start IPTp-SP. We conclude that the toolkit is useful to prompt providers to calculate GA and offer IPTp as early as possible in the second trimester.
Future potential directions include revision of all Toolkit components to reflect input from this evaluation, including development of a wall poster version to enhance readability, and inclusion of a pregnancy wheel to facilitate calculation of GA and estimated date of delivery.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Communication &Health Workers &IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2017
Results from a Formative Evaluation of the Malaria in Pregnancy Case Management Job Aid in Nigeria
Job Aids can provide valuable assistance to health workers, but it is important to evaluate if they serve the intended purpose. With support from USAID’s Maternal and Child Survival Program, Bright Orji, Enobong Ndekhedehe, Elana Fiekowsky, Patricia Gomez, Aimee Dickerson, Reena Sethi, Bibian Udeh, Kristin Vibbert, and Robert Sellke reported at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene on their evaluation of a Job Aid for Nigeria on the prevention of malaria in pregnancy as seen below.
 Annually, nearly 7 million pregnant women in Nigeria are at risk of malaria in pregnancy (MIP). Although antenatal care is the platform for the prevention and treatment of MIP, malaria is also treated at outpatient departments.
Annually, nearly 7 million pregnant women in Nigeria are at risk of malaria in pregnancy (MIP). Although antenatal care is the platform for the prevention and treatment of MIP, malaria is also treated at outpatient departments.
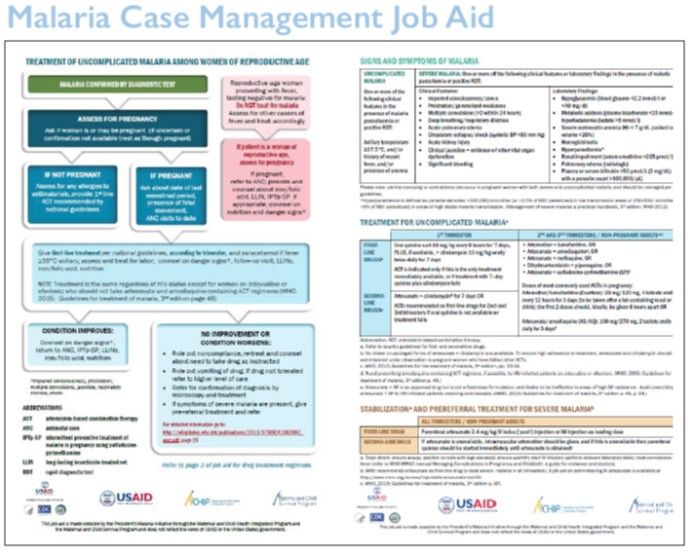
It is known that women of reproductive age (WRA) are often treated for malaria without assessing pregnancy status, although artemisinin combination therapies are contraindicated in the first trimester of pregnancy, and many pregnant women do not receive the recommended low cost interventions.
 In order to increase access to these MIP interventions, the President’s Malaria Initiative supported the Maternal and Child Survival Program and partners to develop a two-page job aid for case management of uncomplicated malaria among WRA. In collaboration with the Nigeria Malaria Elimination Program, the job aid was evaluated in Ebonyi State, a high malaria burden area, to determine providers’ perceptions of its clarity, acceptability, and utility.
In order to increase access to these MIP interventions, the President’s Malaria Initiative supported the Maternal and Child Survival Program and partners to develop a two-page job aid for case management of uncomplicated malaria among WRA. In collaboration with the Nigeria Malaria Elimination Program, the job aid was evaluated in Ebonyi State, a high malaria burden area, to determine providers’ perceptions of its clarity, acceptability, and utility.
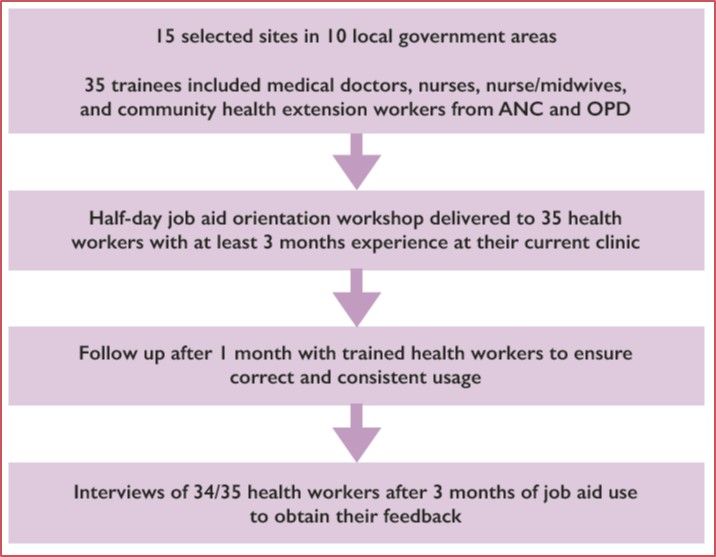
 A half-day workshop on use of the job aid was provided to 35 health workers (nurses – 20%; nurse-midwives – 20%; community health extension workers – 48%; and medical doctors – 12%) already trained on MIP case management, selected from 15 facilities where WRA seek care. After 3 months of use, a one-page questionnaire was administered to 34 health workers.
A half-day workshop on use of the job aid was provided to 35 health workers (nurses – 20%; nurse-midwives – 20%; community health extension workers – 48%; and medical doctors – 12%) already trained on MIP case management, selected from 15 facilities where WRA seek care. After 3 months of use, a one-page questionnaire was administered to 34 health workers.
One-hundred percent stated that the job aid helped them to do the following: identify pregnant women among the WCBA presenting with fever; use rapid diagnostic tests to diagnose malaria; and treat uncomplicated MIP. Sixty-eight percent used the job aid to provide correct treatment for severe malaria and 88% used it while providing services all or most of the time.
The results indicated that after a half-day orientation on use of the job aid, health workers were able to use it to help them identify women who may be pregnant and provide appropriate treatment for uncomplicated MIP. They are also able to explain its use to colleagues.
It is suggested that a poster-size version could be printed and disseminated to appropriate cadres of health workers in clinics where WRA seek care for fever, as it is anticipated that providers could benefit from its use.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Health Workers &Quality of Services Bill Brieger | 09 Nov 2017
Strengthening Nursing & Midwifery Training Through Implementation of Continuous Quality Improvement Process in Tanzania
Annamagreth Mukwenda, John George, Mary Rose Giatas, Gustav Moyo, and Justine Ngenda have been promoting Continuous Quality Improvement and mentoring with nurses and midwives in Tanzania. They shared their experiences working with the Maternal and Child Survival Program and Tanzanian Government agencies at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
 Tanzania is one of the countries with critical shortage of human resource for health. The coverage of skilled birth attendants is about 50%, which connote sub-optimal quality of care contributing to poor neonatal and maternal outcomes.
Tanzania is one of the countries with critical shortage of human resource for health. The coverage of skilled birth attendants is about 50%, which connote sub-optimal quality of care contributing to poor neonatal and maternal outcomes.
 Training and deploying adequate numbers of competent health workers is one of the objectives of the Tanzania National Health Policy. The government of Tanzania and partners like Jhpiego led Maternal and Child Health Survival Program, are working to improve the training environment hence competent graduates.
Training and deploying adequate numbers of competent health workers is one of the objectives of the Tanzania National Health Policy. The government of Tanzania and partners like Jhpiego led Maternal and Child Health Survival Program, are working to improve the training environment hence competent graduates.
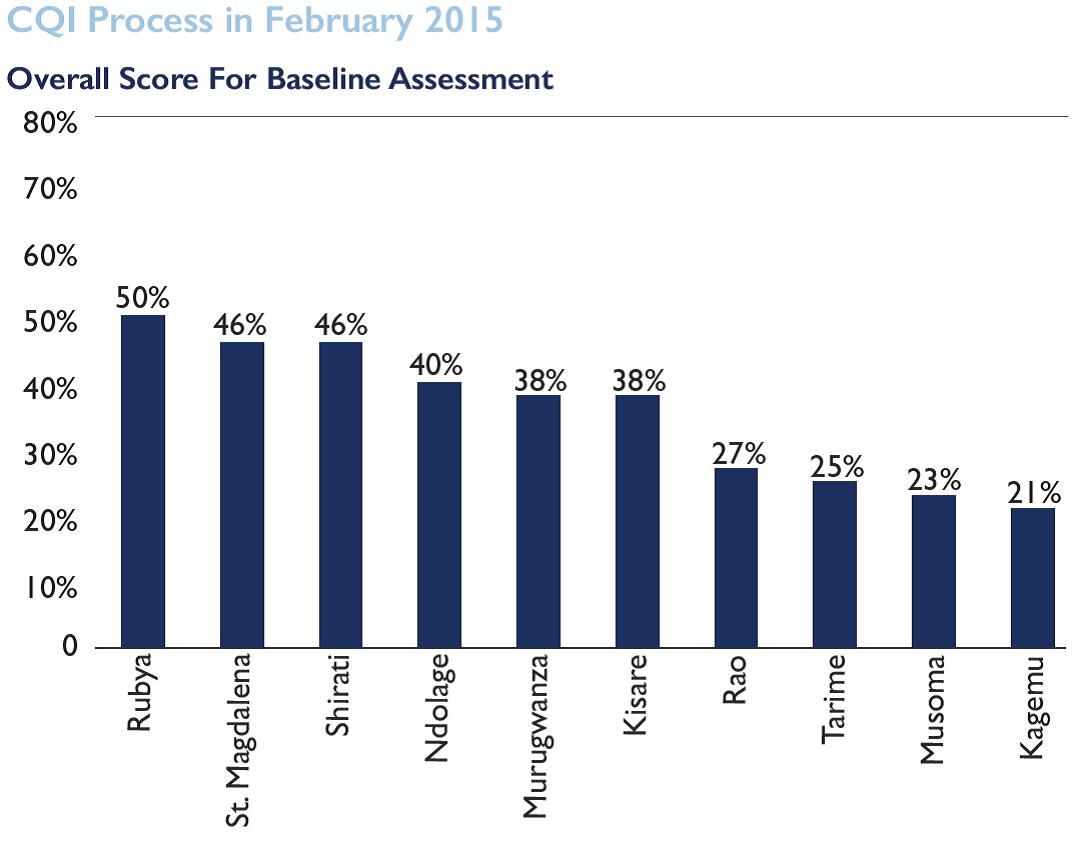
In support of quality trainings, Jhpiego in collaboration with the Ministry of Health are implementing the Continuous Quality Improvement (CQI) process which encourages health training institutions to improve quality teaching and learning by focusing on Classroom and Practical Instructions, Clinical instruction and practice, Institutional Infrastructure, Learning and Teaching Materials and Institutional Governance and Administration.
 A baseline assessment was done using the CQI guide in 10 training institutions to assess the quality of training and educational process, output and outcomes for the provision of quality nursing and midwifery care. Results indicated substandard outcomes with scores less than 50% at most schools.
A baseline assessment was done using the CQI guide in 10 training institutions to assess the quality of training and educational process, output and outcomes for the provision of quality nursing and midwifery care. Results indicated substandard outcomes with scores less than 50% at most schools.
All 10 schools were oriented on CQI process including its implementation. Quarterly assessment by a team comprised of institutions’ quality improvement teams, Ministry of Health and Jhpiego were done and gaps identified addressed through supportive supervision and mentorship.
 Training institution are progressively improving their training capabilities. The teaching learning environment has improved substantially with an average score 95% during external verification from 45% baseline score. After eighteen months of program implementation, three schools have been recognized for their outstanding performance and were presented with trophies and certificates as a motivation. This translates into increased number of skilled health care workers from rural nursing schools with required competency to avert maternal and neonatal deaths.
Training institution are progressively improving their training capabilities. The teaching learning environment has improved substantially with an average score 95% during external verification from 45% baseline score. After eighteen months of program implementation, three schools have been recognized for their outstanding performance and were presented with trophies and certificates as a motivation. This translates into increased number of skilled health care workers from rural nursing schools with required competency to avert maternal and neonatal deaths.
Case Management &Health Workers &IPTp &Quality of Services Bill Brieger | 08 Nov 2017
Contribution of the Standards-Based Management and Recognition (SBM-R) approach to fighting malaria in Burkina Faso
Quality improvement tools play an important role in ensuring better malaria services. Moumouni Bonkoungou, Ousmane Badolo, and Thierry Ouedraogo describe how

Standards Based Management and Recognition Approach to Quality Improvement
Jhpiego’s quality approach, Standards-Based Management and Recognition, was applied to enhancing the provision of malaria services in Burkina Faso at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their work was supported through the President’s Malaria Initiative and the USAID Improving Malaria Care Project.
In 2015, Burkina Faso recorded 8,286,463 malaria cases, including 450,024 severe cases with 5379 deaths. The main reasons for these death are: Inadequate application of national malaria diagnosis and treatment guidelines, delays in seeking health care and poor quality of case management.
The Standards-Based Management and Recognition (SBM-R) approach is used to improve quality of care using performance standards based on national guidelines. SBM-R includes the following steps:
- set performance standards
- implement the standards
- monitor progress and
- recognize as well as celebrate achievements
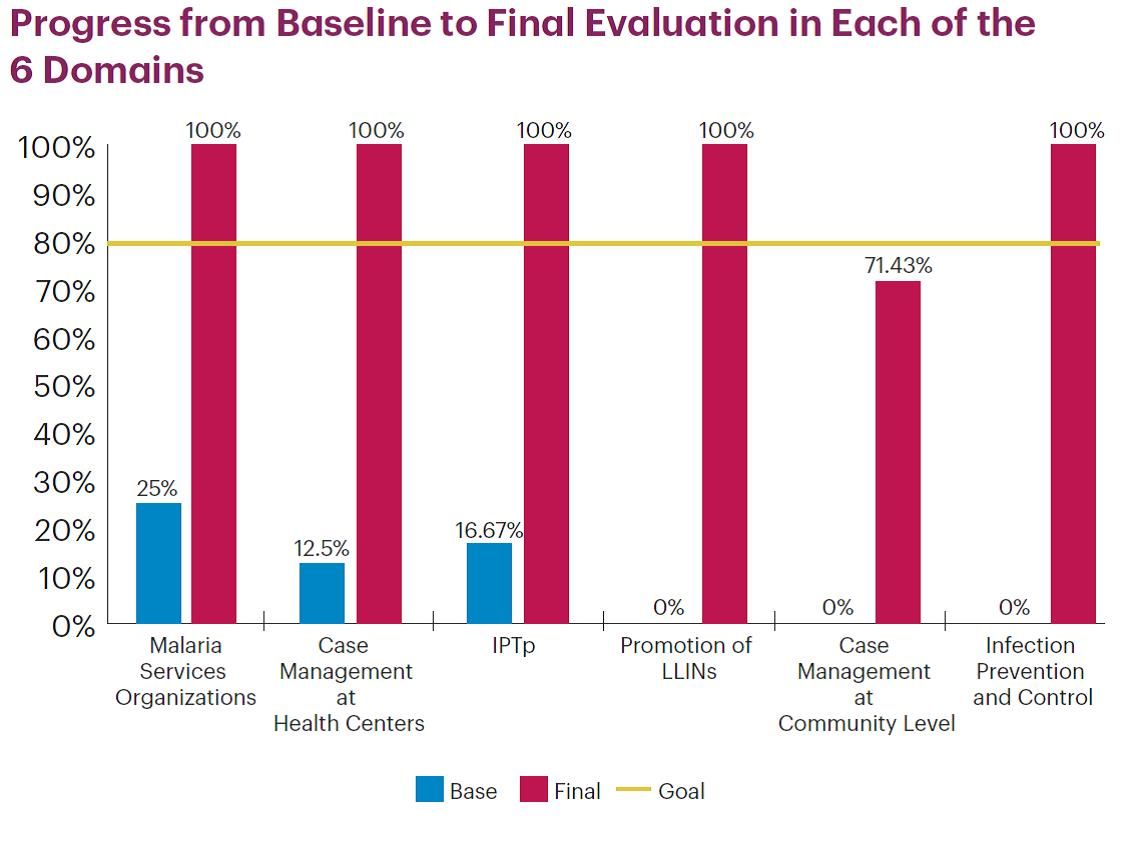 Areas or domains assessed by the approach are: services organization, case management at both health center and community, Intermittent Preventive Treatment in Pregnancy (IPTp), promotion of Long Lasting Insecticide treated Nets (LLIN) use and infection prevention and control.
Areas or domains assessed by the approach are: services organization, case management at both health center and community, Intermittent Preventive Treatment in Pregnancy (IPTp), promotion of Long Lasting Insecticide treated Nets (LLIN) use and infection prevention and control.
Since June 2016, 26 health facilities in three regions have been implementing SBMR. Therefore, 105 health workers have been trained. Performance progress was measured through 5 evaluations including baseline. Baseline has shown the highest score was 47% (Kounda) while the lowest was 9% (Niangoloko).
The main issues observed were: lack of program activities, management tools, handwashing facilities, LLINs and misuse of Rapid Diagnosis Tests. Their cause was determined and an improvement plan was developed by each site. The second, third and final evaluations revealed a change in performance scores for all sites.
 The external evaluation showed 17 out of 26 health facilities with a score higher than 60%; among them 10 with a score above 80% (Bougoula, 94%). At the same time, IPTp 3 increased from 34.48% in 2014 to 78.38% in 2016 and no malaria death has been registered since October 2015.
The external evaluation showed 17 out of 26 health facilities with a score higher than 60%; among them 10 with a score above 80% (Bougoula, 94%). At the same time, IPTp 3 increased from 34.48% in 2014 to 78.38% in 2016 and no malaria death has been registered since October 2015.
For the site under 80% the key reasons were: staff turnover, commodities stock-out and lack of infrastructure. The process continues with recognition of health facilities and supporting others (those at less than 80%) to reach the desired performance level. The SBM-R approach appears to be a great tool for improving quality and performance of health facilities.
Case Management &Health Workers &Training Bill Brieger | 08 Nov 2017
Health provider orientation to national malaria case management guidelines in regional hospitals in Burkina Faso
 Good clinical practice in managing malaria requires awareness and understanding of national case management guidelines. Moumouni Bonkoungou, Ousmane Badolo, and Thierry Ouedraogo of Jhpiego in Collaboration with the National Malaria Control Program and sponsorship from the “Improving Malaria Care” project of USAID/PMI explain how health workers in Burkina Faso were oriented to the national guidelines at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. They have found that short orientations are less expensive and reach more health workers that traditional training sessions.
Good clinical practice in managing malaria requires awareness and understanding of national case management guidelines. Moumouni Bonkoungou, Ousmane Badolo, and Thierry Ouedraogo of Jhpiego in Collaboration with the National Malaria Control Program and sponsorship from the “Improving Malaria Care” project of USAID/PMI explain how health workers in Burkina Faso were oriented to the national guidelines at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. They have found that short orientations are less expensive and reach more health workers that traditional training sessions.
Malaria remains the leading cause of consultations, hospitalization and death in health facilities in Burkina Faso. In 2015, 23,634 cases of severe malaria were recorded in hospitals with 1,634 deaths, a mortality rate of 7% at this level compared to 1% nationally. Since April 2014, 1,819 providers from 49 districts have been trained in malaria case management, specifically at the first level (health center – CSPS). Conversely, at referral centers – medical centers with surgical units (CMA), regional hospitals (CHR) and university hospitals (CHU) – providers are not well educated on the new WHO guidelines for malaria prevention and case management.

Health worker orientation session
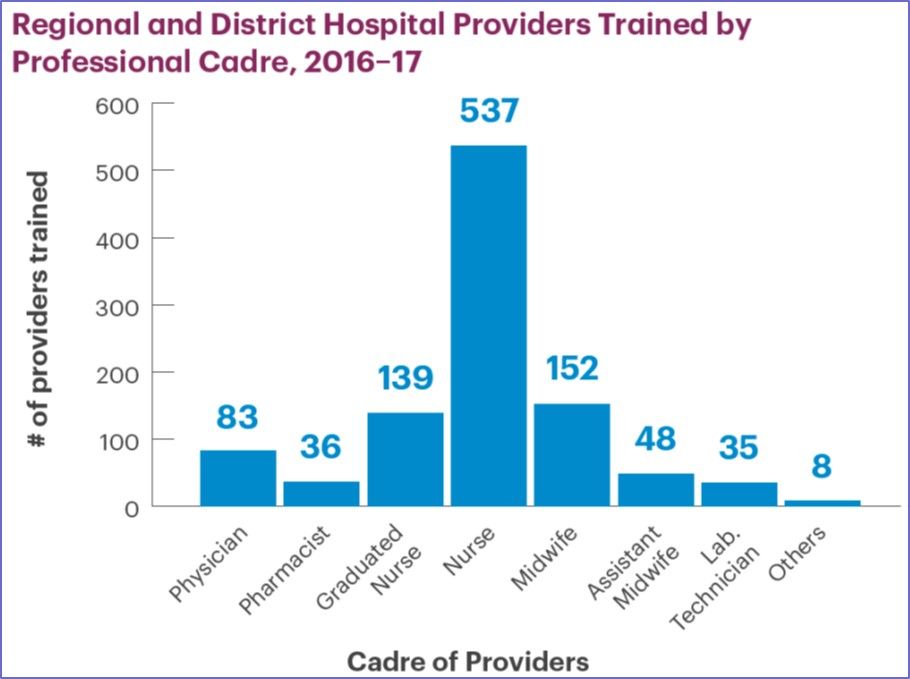
This situation led the United States Agency for International Development-supported Improving Malaria Care (IMC) project and the National Malaria Control Program (NMCP) to organize orientation sessions for providers in 8 CHR in September 2016. The sessions were conducted by trainers at the national level, supported by clinicians from hospitals including pediatricians and gynecologists.
A total of 298 health workers were oriented, including 24 physicians, 157 nurses, 56 midwives, as well as pharmacists and laboratory technicians. 39% of participants were female and 43% have less than 5 years of service in these hospitals. The sessions have provided participants with an opportunity to familiarize themselves with the new guidelines for malaria prevention and case management.
 The orientations have also made it possible to identify the difficulties encountered by referral structures in malaria case management, which include: insufficient staff, inadequate capacity building, no blood bank in some hospitals, reagent stock-outs, inadequacies in the referral system, and insufficient equipment.
The orientations have also made it possible to identify the difficulties encountered by referral structures in malaria case management, which include: insufficient staff, inadequate capacity building, no blood bank in some hospitals, reagent stock-outs, inadequacies in the referral system, and insufficient equipment.
To address these difficulties, staff redeployment, internal supervision, development of tools to monitor reagents stocks have been proposed. To move forward, response plans for the period of high malaria transmission is expected to be developed for these referral facilities.
Health Workers &Human Resources &IPTp &Training &Treatment Bill Brieger | 07 Nov 2017
Using rapid task analysis to strengthen Pre-Service Education (PSE) learning and performance of critical malaria interventions in Liberia
 Understanding the tasks that health workers perform in real life can improve their basic Training. Marion Subah of MCSP and Jhpiego shares experiences in using Task Analysis to improve pre-service training of midwives and lab technicians in Liberia. Her findings summarized below, are presented at the American Society of Tropical Medicine’s 66th Annual Meeting.
Understanding the tasks that health workers perform in real life can improve their basic Training. Marion Subah of MCSP and Jhpiego shares experiences in using Task Analysis to improve pre-service training of midwives and lab technicians in Liberia. Her findings summarized below, are presented at the American Society of Tropical Medicine’s 66th Annual Meeting.
Health worker task analysis helps human resource planners and managers update pre-service education (PSE) curricula and plan needed in- service training. In Liberia, a task analysis was conducted focusing on Liberia’s midwives’ and Medical Laboratory Technicians’ (MLT) work practices.
service training. In Liberia, a task analysis was conducted focusing on Liberia’s midwives’ and Medical Laboratory Technicians’ (MLT) work practices.
Task lists were developed using curricula, job descriptions and professional scope of practice, and validated by key stakeholders for each cadre. Responses from 25 MLTs and 26 midwives were examined that addressed the following questions:
- How often do you do the task (frequency)?
- Where did you learn to do the task (location)?
- How well do you think you are able to perform the task (performance)?
- How critical is the task in terms of patient and/or public health outcomes (criticality).
 Eligibility criteria included those currently practicing between 6 months and 5.5 years following graduation. Midwives were assessed for five tasks relating to malaria service provision, including provision of preventive treatment for malaria in pregnancy, management of vector borne diseases, diagnosis and management uncomplicated malaria in adults and children (respectively), and provision of malaria preventive services.
Eligibility criteria included those currently practicing between 6 months and 5.5 years following graduation. Midwives were assessed for five tasks relating to malaria service provision, including provision of preventive treatment for malaria in pregnancy, management of vector borne diseases, diagnosis and management uncomplicated malaria in adults and children (respectively), and provision of malaria preventive services.
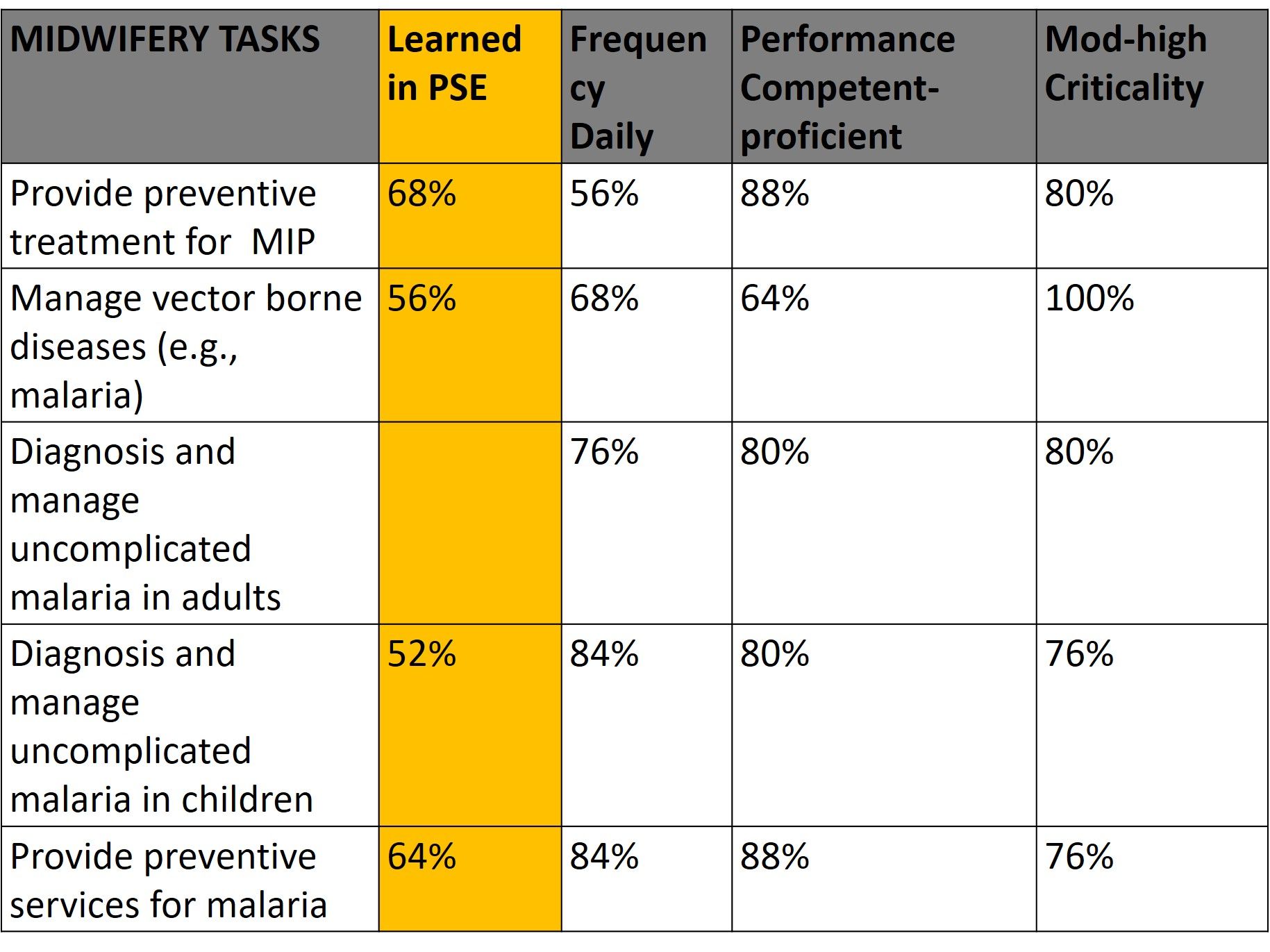 Lab technicians were assessed for one malaria task, performance of parasitological tests. On average 61% of midwives learned these malaria tasks in PSE, 74% said they performed these tasks daily, 80% felt proficient in performing the tasks, and 82% rated the tasks moderate to high in criticality. For MLTs, 88% learned malaria testing in pre-service education, 100 % performed this task daily, 77% felt they were proficient and 93% said the task was of moderate to high criticality.
Lab technicians were assessed for one malaria task, performance of parasitological tests. On average 61% of midwives learned these malaria tasks in PSE, 74% said they performed these tasks daily, 80% felt proficient in performing the tasks, and 82% rated the tasks moderate to high in criticality. For MLTs, 88% learned malaria testing in pre-service education, 100 % performed this task daily, 77% felt they were proficient and 93% said the task was of moderate to high criticality.
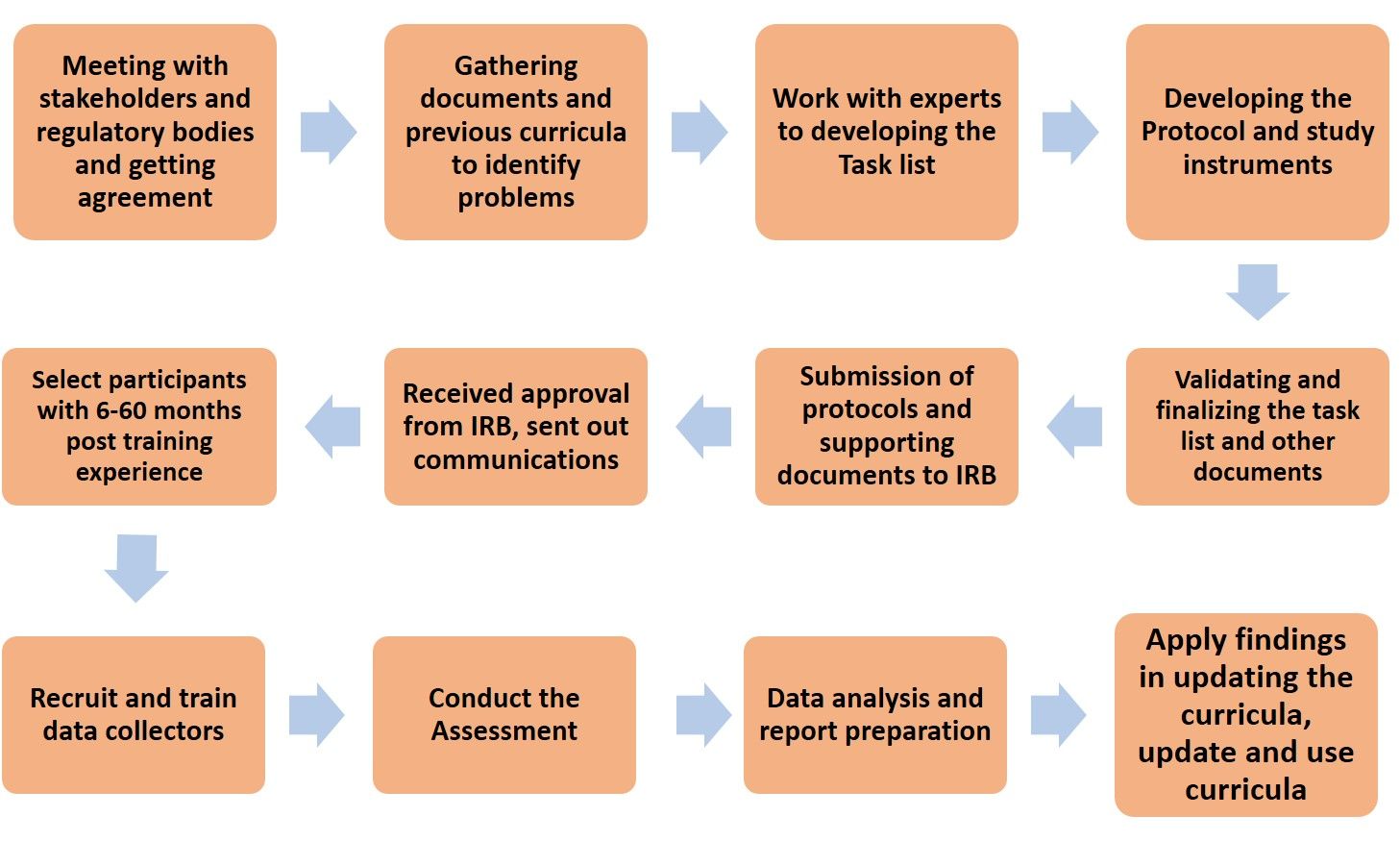
Task Analysis Flow Chart
The results from this rapid task analysis are being applied to the current curricula review. Courses that could be updated or strengthened have been identified. Malaria Case Management Technical Update and Effective Teaching Skills Training are being organized for tutors at the training schools. Finally, integrated supportive supervision tools are being strengthened to improve performance of these malaria tasks by midwives and lab technicians.
Diagnosis &Health Workers &Learning/Training Bill Brieger | 05 Nov 2017
Performance assessment of laboratory technicians on Malaria Microscopy in 5 high endemic districts of Rwanda
 Parasitological diagnosis plays an increasing role in malaria control and elimination. Noella Umulisa, Angelique Mugirente, Tharcisse Munyaneza, Aniceth Rucogoza, Aline Uwimana, Beata Mukarugwiro, Stephen Mutwiwa, Aimable and Mbituyumuremyi of the
Parasitological diagnosis plays an increasing role in malaria control and elimination. Noella Umulisa, Angelique Mugirente, Tharcisse Munyaneza, Aniceth Rucogoza, Aline Uwimana, Beata Mukarugwiro, Stephen Mutwiwa, Aimable and Mbituyumuremyi of the
Maternal and Child Survival Program, Jhpiego, the National Reference Laboratory, Rwanda Biomedical Centre (RBC), and the Malaria and Other Parasitic Diseases Division (Mal & OPDD) in Rwanda will present their experiences building the capacity of lab technicians during Session 47 at the American Society of Tropical Medicine and Hygiene Annual Meeting on 6 November 2017. Their abstract is found below.
Accurate malaria diagnostics help to establish the true prevalence of each Plasmodium species and can ensure appropriate treatment. Light microscopy is the gold standard for malaria diagnosis and sufficient training of laboratory staff is paramount for the correct microscopy diagnosis of malaria. In Rwanda each of about 400 health centers has a laboratory able to perform malaria microscopy, at least 2 trained lab technicians and 1 to 2 functioning microscopes.
The objective of the study is to evaluate the performance of laboratory technicians in detecting and quantifying malaria parasites in 81 health centers from 5 highly endemic districts (Huye, Nyanza, Ngoma, Kirehe, Kayonza, Gatsibo). In October 2015 the Rwanda Biomedical Center and partners trained 1 lab technician per health center from these districts in malaria microscopy.
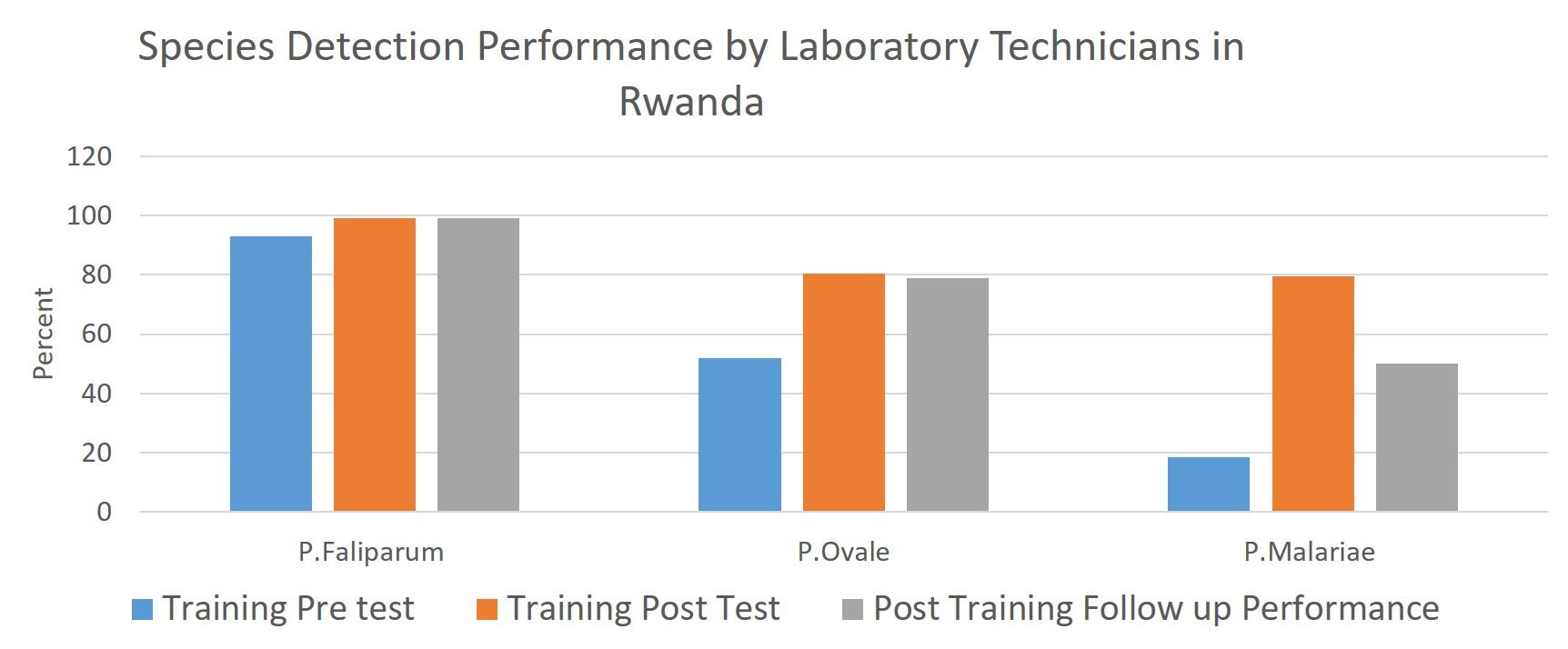 The training emphasized determining parasite density and detection of malaria species. From August to September 2016 a follow-up assessment was conducted. Of the 81 technicians trained, 30 were randomly chosen and assessed at their health facilities.
The training emphasized determining parasite density and detection of malaria species. From August to September 2016 a follow-up assessment was conducted. Of the 81 technicians trained, 30 were randomly chosen and assessed at their health facilities.
A standardized pre-validated slide panel of 5 slides was distributed, a comprehensive checklist used to collect information and conduct visual inspection and maneuvers used in routine malaria diagnosis. During the training a significant increase was found between pre and post tests with median scores improving from 47% to 85%.
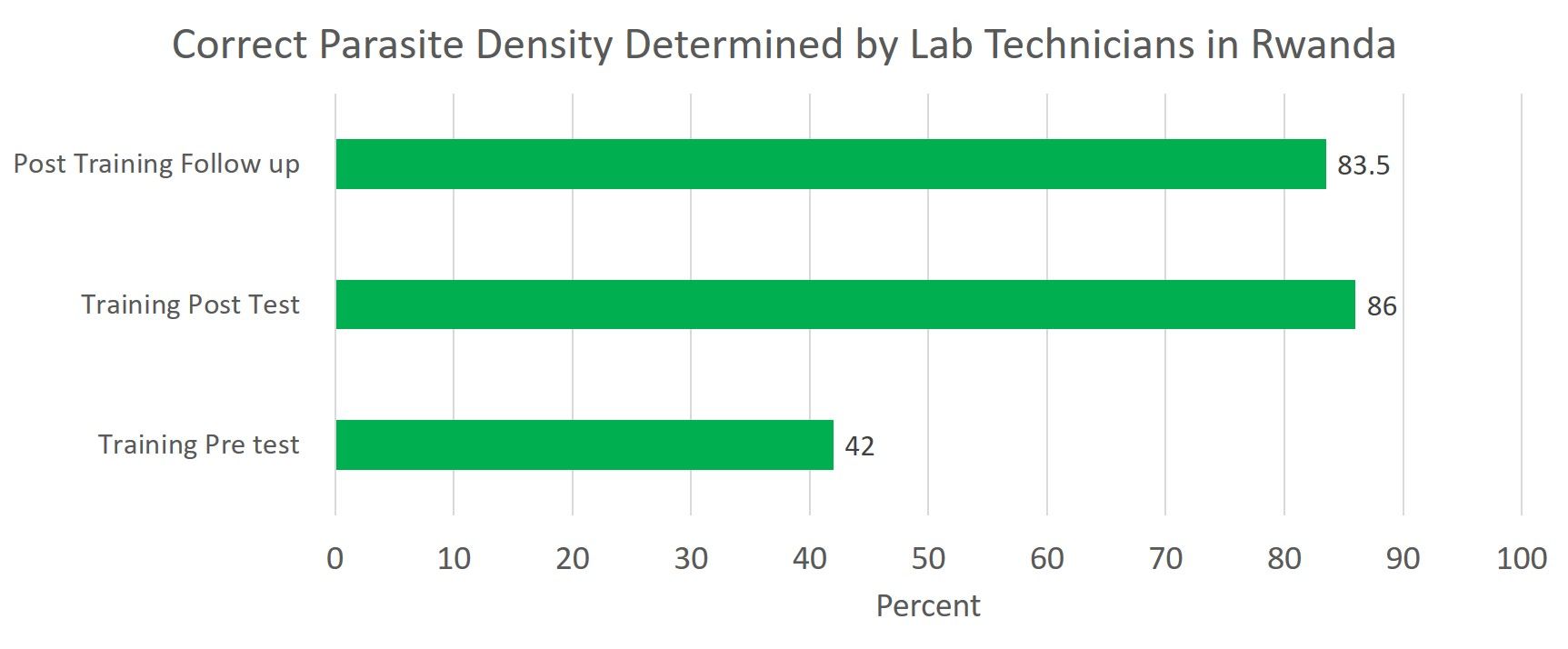 As part of the assessment 150 lab tech-prepared slides were analyzed to evaluate the quality of thick and thin blood smears. There was a significant increase in quality of both blood smear types. The sensitivity and specificity of participants in detection of malaria parasites were 100% and 86% respectively, while species identification and parasite quantification accuracy were 79% and 75% respectively.
As part of the assessment 150 lab tech-prepared slides were analyzed to evaluate the quality of thick and thin blood smears. There was a significant increase in quality of both blood smear types. The sensitivity and specificity of participants in detection of malaria parasites were 100% and 86% respectively, while species identification and parasite quantification accuracy were 79% and 75% respectively.
The findings of this assessment support the need for continuous capacity building for laboratory staff to ensure accurate malaria diagnosis for appropriate treatment and suggest that District hospitals may benefit from conducting regular malaria microscopy diagnosis quality control/assurance activities at health center laboratories.
CHW &Diagnosis &Health Workers &Performance &Training &Treatment Bill Brieger | 06 Apr 2017
World Health Workers Week, a Time to Recognize Health Worker Contributions to Malaria Care
 Since the beginning of the Roll Back malaria Partnership in 1998 there has been strong awareness that malaria control success is inextricably tied to the quality of health systems. Achieving coverage of malaria interventions involves all aspects of the health system but most particularly the human resources who plan, deliver and assess these services. World Health Worker Week is a good opportunity to recognize health worker contributions to ridding the world of malaria.
Since the beginning of the Roll Back malaria Partnership in 1998 there has been strong awareness that malaria control success is inextricably tied to the quality of health systems. Achieving coverage of malaria interventions involves all aspects of the health system but most particularly the human resources who plan, deliver and assess these services. World Health Worker Week is a good opportunity to recognize health worker contributions to ridding the world of malaria.
We can start with community health workers who may be informal but trained volunteers or front line formal health staff. According to the Frontline Health Workers Coalition, “Frontline health workers provide immunizations and treat common infections. They are on the frontlines of battling deadly diseases like Ebola and HIV/AIDS, and many families rely on them as trusted sources of information for preventing, treating and managing a variety of leading killers including diarrhea, pneumonia, malaria and tuberculosis.”
 The presence of CHWs exemplifies the ideal of a partnership between communities and the health system. With appropriate training and supervision CHWs ensure that malaria cases are diagnosed and treated promptly and appropriately, malaria prevention activities like long lasting insecticide-treated nets are implemented and pregnant women are protected from the dangers of the disease. CHWs save lives according to Nkonki and colleagues who “found evidence of cost-effectiveness of community health worker (CHW) interventions in reducing malaria and asthma, decreasing mortality of neonates and children, improving maternal health, increasing exclusive breastfeeding and improving malnutrition, and positively impacting physical health and psychomotor development amongst children.”
The presence of CHWs exemplifies the ideal of a partnership between communities and the health system. With appropriate training and supervision CHWs ensure that malaria cases are diagnosed and treated promptly and appropriately, malaria prevention activities like long lasting insecticide-treated nets are implemented and pregnant women are protected from the dangers of the disease. CHWs save lives according to Nkonki and colleagues who “found evidence of cost-effectiveness of community health worker (CHW) interventions in reducing malaria and asthma, decreasing mortality of neonates and children, improving maternal health, increasing exclusive breastfeeding and improving malnutrition, and positively impacting physical health and psychomotor development amongst children.”
 CHWs do not act in isolation but depend on health workers at the facility and district levels for training, supervision and maintenance of supplies and inventories. These health staff benefit from capacity building – when they are capable of performing malaria tasks, they can better help others learn and practice.
CHWs do not act in isolation but depend on health workers at the facility and district levels for training, supervision and maintenance of supplies and inventories. These health staff benefit from capacity building – when they are capable of performing malaria tasks, they can better help others learn and practice.
A good example of this capacity building is the Improving Malaria Care (IMC) project in Burkina Faso, implemented by Jhpiego and supported by USAID and the US President’s malaria Initiative. IMC builds capacity of health workers at facility and district level to improve malaria prevention service delivery and enhance accuracy in malaria diagnosis and treatment. Additionally capacity building is provided to health staff in the National Malaria Control Program to plan, design, manage and coordinate a comprehensive malaria control program. As a result of capacity building there has been a large increase in malaria cases diagnosed using parasitological techniques and in the number of women getting more doses of intermittent preventive treatment to prevent malaria during pregnancy.
Malaria care is much more than drugs, tests and nets. Health worker capacity is required to get the job done and move us forward on the pathway to eliminate malaria.