Health Information &Malaria in Pregnancy Bill Brieger | 07 Nov 2017
Improving Quality of Data to Advance Malaria in Pregnancy Indicator Coverage in Ebonyi State, Nigeria
Progress in preventing malaria in pregnancy depends on good data. Bright Orji, Gladys Olisaekee, Onyinye Udenze, Enobong Umoekeyo, Chika Nwankwo, Boniface Onwe, Chibugo Okoli, and Emmanuel Otolorin of Jhpiego discussed ways to improve data quality in Nigeria at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene with support from the USAID Maternal and Child Health Program. A summary of their points follows:

Reviewing Health Facility Data
Quality data are crucial for informed decision-making to address health challenges and improve malaria service delivery among countries on the pathway to malaria elimination. This emphasis on better data quality was reflected in the World Malaria Day theme of “Counting Malaria Out” in 2009 and 2010.
In Nigeria, improving malaria data quality has been difficult due to critical health system challenges including poor coordination across different departments, institutional complexities, and a shortage of medical record officers and service providers sufficiently trained in data visualization and use of data for decision-making. In response, the Maternal and Child Health Survival Program (MCSP) in Nigeria embarked on the implementation of key activities to improve quality of malaria data in Ebonyi State.
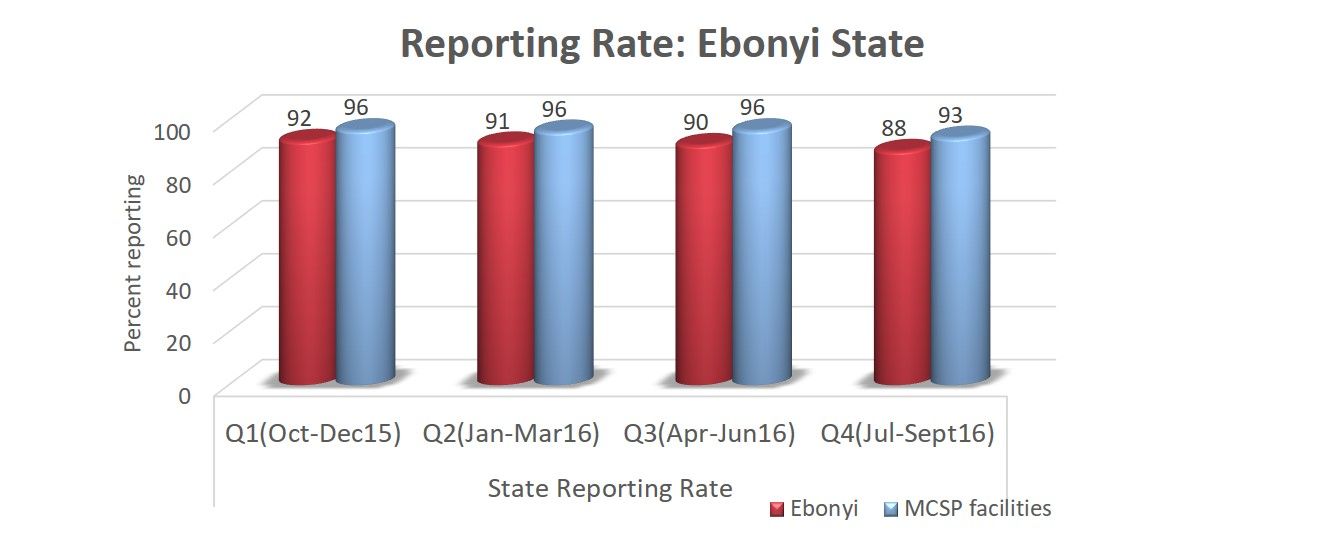 These activities included training on record keeping and use of data for decision-making; post training follow-up; dash boards at the frontline for better data visualization; monthly data collation meetings; improved synergy among service departments; and quarterly data quality assurance visits. As a result, more than 75% of facilities graphed malaria indicators thereby increasing data visualization and use of data for decision-making.
These activities included training on record keeping and use of data for decision-making; post training follow-up; dash boards at the frontline for better data visualization; monthly data collation meetings; improved synergy among service departments; and quarterly data quality assurance visits. As a result, more than 75% of facilities graphed malaria indicators thereby increasing data visualization and use of data for decision-making.
An example of data improvements leading to service increases was Intermittent Preventive Treatment for malaria in pregnancy (IPTp). IPTp1 service statistics in MCSP-supported facilities improved from 54.1% in Oct-Dec 2015 to 81.3% by Jul-Sept 2016 compared to 54.7% to 67.8% in the same periods for non-MCSP facilities.
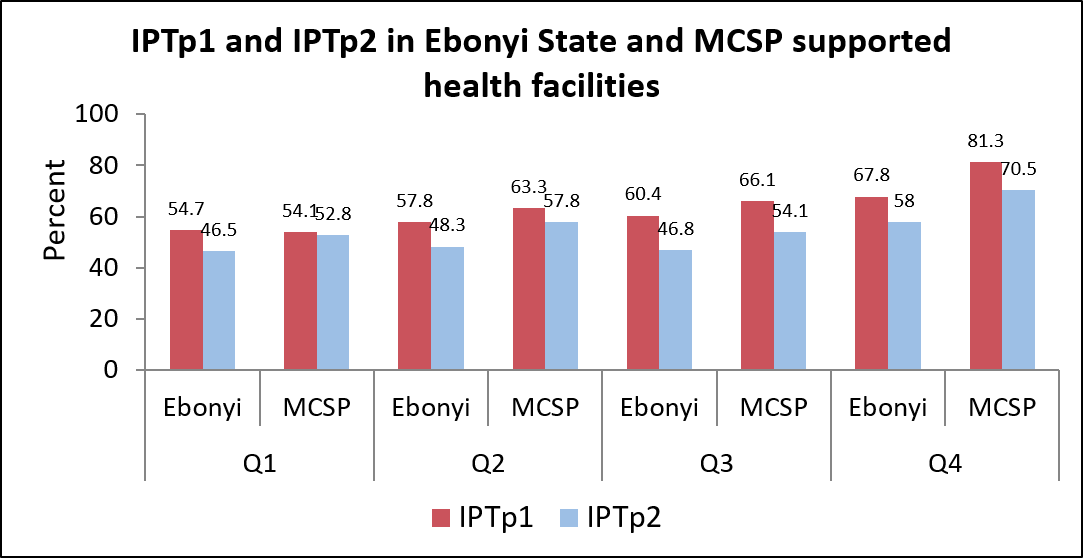 Similarly, IPTp2 service statistics in MCSP-supported facilities improved from 52.8% to 70.5%compared to 46.5% to 58.0% in the same period for non-MCSP facilities.
Similarly, IPTp2 service statistics in MCSP-supported facilities improved from 52.8% to 70.5%compared to 46.5% to 58.0% in the same period for non-MCSP facilities.
Data quality improvement interventions such as monthly data collation and validation meetings prior uploading data to DHIS can contribute to improved quality of malaria performance indicators, better coordination between antenatal care, outpatient and pharmacy departments and increased IPTp coverage.
Health Information &IPTp &Malaria in Pregnancy Bill Brieger | 13 Nov 2016
Collaborative efforts to improve prevention of malaria in pregnancy in Burkina Faso through use of IPTp-SP
Mathurin Dodo, Stanislas Paul Nebie, Ousmane Badolo, Thierry Ouedraogo, Rachel Waxman, Danielle Burke, William R. Brieger, and Elaine Roman of Jhpiego’s USAID sponsored Improving Malaria Care project based in Ouagadougou, Burkina Faso will be presenting a poster on improving intermittent treatment of malaria in pregnancy at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene on Monday 14th November in Atlanta. Their Abstract follows:

Ensuring the inclusion of IPTp3 doses and higher in the national health information system enabled documentation of improved coverage
Malaria remains the first cause of consultation (47%), hospitalization (62%) and death (31%) in health facilities in Burkina Faso (2014 Statistical Yearbook). Pregnant women are among the most vulnerable to malaria. Intermittent preventive treatment in pregnancy (IPTp) is a priority intervention in the Burkina Faso 2011-2015 National Malaria Strategic Plan. In 2012, IPTp2 was low across the country at 53%.
The President’s Malaria Initiative (PMI) supported the National Malaria Control Program (NMCP) in implementing the national malaria control strategic plans. IPTp was promoted through 3 strategies: advocacy and policy updates, capacity building, and behavior change communication. Malaria prevention and management guidelines and job aids updated stressed IPTp in line with WHO recommendations.
 185 trainers were trained who in turn organized one-day briefings for over 1,300 healthcare providers from 1081 health facilities (61.3% of health facilities nationally) on the revised guidelines, which were distributed along with job aids. Health information system tools now reflect new IPTp guidance, and 190 district and regional level data managers were trained in their use.
185 trainers were trained who in turn organized one-day briefings for over 1,300 healthcare providers from 1081 health facilities (61.3% of health facilities nationally) on the revised guidelines, which were distributed along with job aids. Health information system tools now reflect new IPTp guidance, and 190 district and regional level data managers were trained in their use.
208 community health workers were trained in sensitization and community mobilization around early ANC attendance. Over 3000 radio and TV spots were aired on 28 stations on the importance of IPTp.
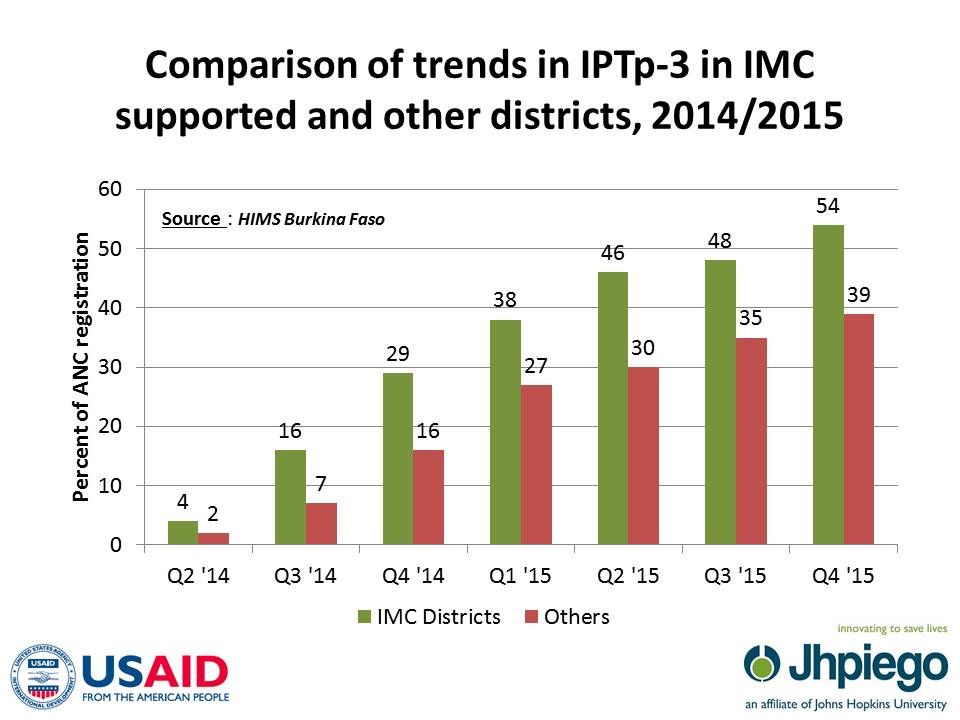
 In 21 project districts in 2013, IPTp2 and IPTp3 coverage rates based on ANC registration were 54% and 0%. Following the interventions, rates in these districts increased to 72% (IPTp2) and 23% (IPTp3) in 2014 compared to 63% and 8% in the other 42 districts.
In 21 project districts in 2013, IPTp2 and IPTp3 coverage rates based on ANC registration were 54% and 0%. Following the interventions, rates in these districts increased to 72% (IPTp2) and 23% (IPTp3) in 2014 compared to 63% and 8% in the other 42 districts.
These efforts have resulted in improvements in IPTp service delivery and reporting. Based on successes, training and guideline dissemination continued in 2015 across the country so that all health facilities received copies of the new guidelines and 82% of districts received training.
Health Information &Monitoring Bill Brieger | 22 Jun 2014
Regular data Review Meetings in Mozambique, a Path to Improving Malaria Service Delivery
Health Alliance International (HAI) of the University of Washington, is collaborating with Centro de Investigação Operacional da Beira (CIOB) is based in Beira, Mozambique to improve the quality and use of routine monitoring and evaluation data from the health facility through to the district in Sofala Province. The aim is to strengthen the health system through data for decision making and improve quality and uptake of services. This effort is sponsored by a grant from the Doris Duke Charitable Foundation.
 A key feature of the program is a regular data review meeting where representatives from health facilities in a district come together and each presents his/her standard Ministry of Health service indicators in a simple slide format. After each presentation the speaker received feedback from the group, including members of the district health management team, on successes and challenges and is encouraged to make plans to improve both data quality and service uptake.
A key feature of the program is a regular data review meeting where representatives from health facilities in a district come together and each presents his/her standard Ministry of Health service indicators in a simple slide format. After each presentation the speaker received feedback from the group, including members of the district health management team, on successes and challenges and is encouraged to make plans to improve both data quality and service uptake.
The data review meetings started with an overview of all HIV, reproductive, maternal and child health indicators. Separate review meetings for malaria service indicators have been recently introduced.
According to members of the district teams, the individual facility staff presenters have grown more skilled in formatting their data and presenting to an audience. Overall, participants in these meetings appear enthusiastic and interested in the results of their peers. Constructive critiques are the norm, and speakers express appreciation for suggestions on how they can improve their services and the resulting data.
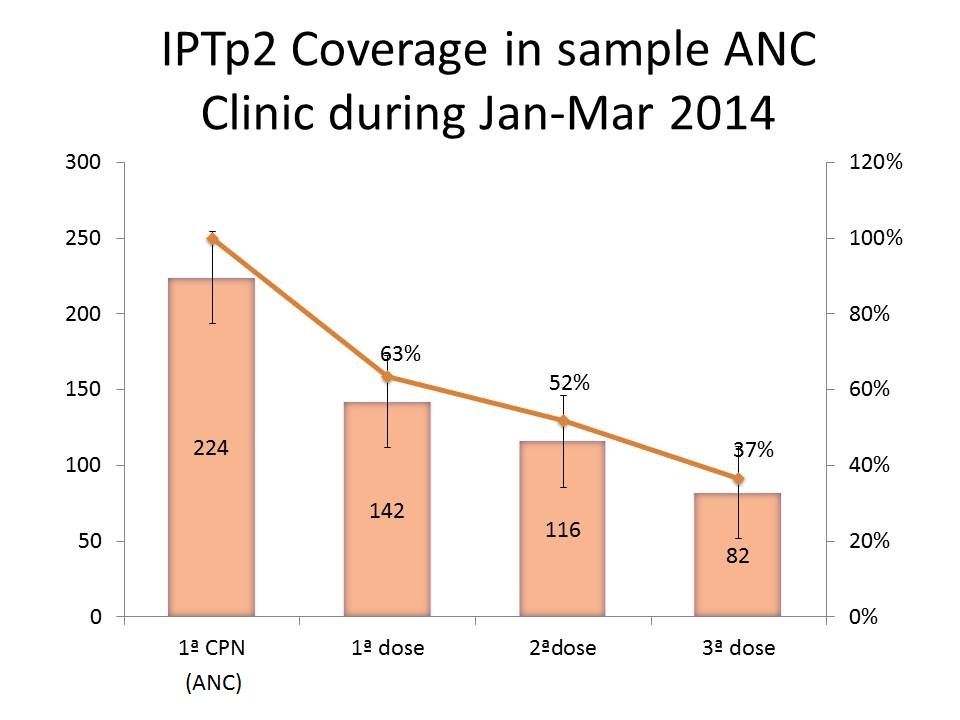 A sample chart from a health facility showing a quarterly review of intermittent preventive treatment for malaria in pregnancy (IPTp) is seen to the right. After viewing this, meeting participants might ask the presenter what are the reasons for the drop-off in coverage. If for example, the problem of late antenatal care (ANC) attendance is mentioned, the group can ask the presenter to consider how to encourage women to attend earlier.
A sample chart from a health facility showing a quarterly review of intermittent preventive treatment for malaria in pregnancy (IPTp) is seen to the right. After viewing this, meeting participants might ask the presenter what are the reasons for the drop-off in coverage. If for example, the problem of late antenatal care (ANC) attendance is mentioned, the group can ask the presenter to consider how to encourage women to attend earlier.
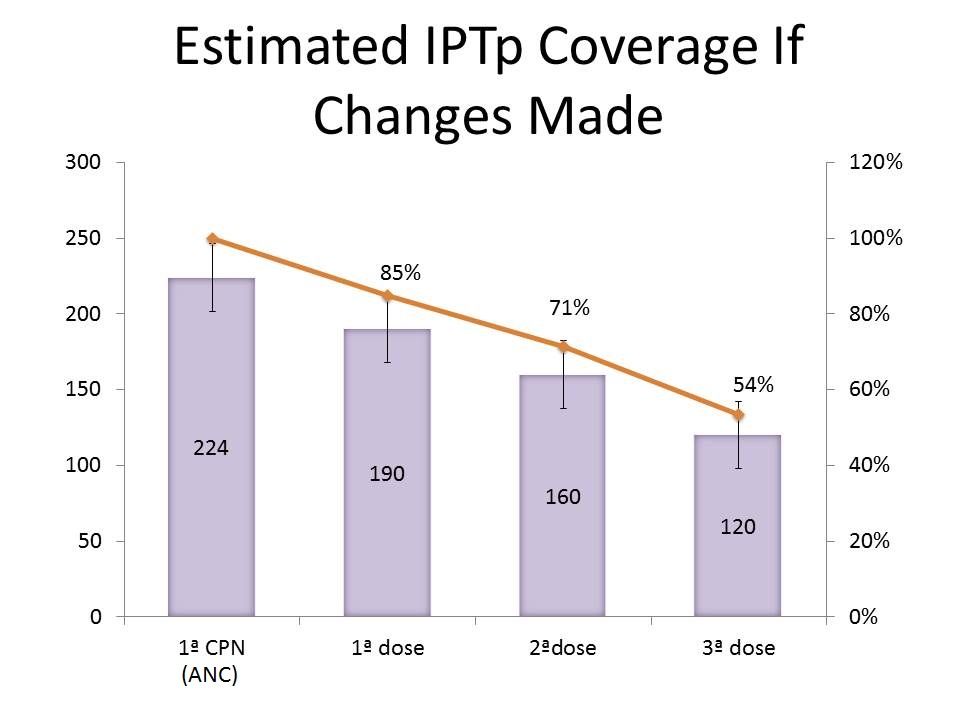 If the presenter then goes back and implements the suggestions, the second chart might reflect the results of improved service uptake. In this way the overall project hopes that close examination of their own data by service providers can strengthen service delivery and the health system.
If the presenter then goes back and implements the suggestions, the second chart might reflect the results of improved service uptake. In this way the overall project hopes that close examination of their own data by service providers can strengthen service delivery and the health system.
We look forward to hearing more about this unique process so that it can be disseminated in other malaria endemic countries.
Epidemiology &Health Information &Monitoring &Surveillance Bill Brieger | 26 Apr 2014
iPhones for household malaria surveys in Sierra Leone
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of a poster presented by Suzanne Van Hull of Catholic Relief Services.
Catholic Relief Services (CRS) and the Ministry of Health and Sanitation (MoHS) of Sierra Leone (SL) are co-implementing nationwide malaria prevention and treatment activities funded by the Global Fund to fight AIDS, Tuberculosis and Malaria. In order to track progress and impact, CRS and partners led the implementation of a malaria indicator survey (MIS) in early 2013 covering a nationally-representative sample of 6,720 households, inclusive of blood testing to determine prevalence of anemia and malaria. In early 2012, CRS also had the experience of using mobile technology for a Knowledge Attitude and Practices (KAP) study.
Fieldworkers used Apple 3GS iPhones for both surveys to collect data via the iFormBuilder platform, a web-based, software-as-services application with a companion app for the mobile devices allowing for timely data collection, monitoring, and analysis.
This was the first time that iPhones were used for a MIS, and lessons learned include: allowing at least four months to transform paper-based questionnaires into electronic format, giving the program enough time for pre-testing the tool and training data collectors/biomarkers/laboratory technicians, and involving key malaria stakeholders to ensure a nationally-led survey. Global Positioning Systems enabled the MoHS to make in-depth analyses on malaria trends based on geographic locations.
 Overall the benefits of an electronic versus a paper-based MIS questionnaire outweighed the challenges. The iPhone technology eliminated the need for paper transcribing, allowing for quicker data tabulation, real-time identification of mistakes, faster interviewing through skip patterns, and a close-to-clean dataset by the end of data collection saving time and money.
Overall the benefits of an electronic versus a paper-based MIS questionnaire outweighed the challenges. The iPhone technology eliminated the need for paper transcribing, allowing for quicker data tabulation, real-time identification of mistakes, faster interviewing through skip patterns, and a close-to-clean dataset by the end of data collection saving time and money.
Survey results will be used to set evidence-based targets for all partners’ future malaria activities, especially the next 3 years of GF-supported malaria grants
Health Information &Treatment Bill Brieger | 27 Oct 2011
Cambodia DHS lacks adequate attention to malaria
 The Cambodia Demographic and Health Survey 2010 report is now available for download.
The Cambodia Demographic and Health Survey 2010 report is now available for download.
Surprisingly little information is available about malaria. The following narrative on ‘fever’ was provided:
“Less than 1 percent of children with fever received antimalarial drugs, whereas 44 percent received antibiotic drugs. Use of antibiotic drugs was more common in urban areas (52 percent) than in rural areas (43 percent) and more common among mothers with at least a secondary education (54 percent) than among mothers with no schooling (39 percent). Mothers in Prey Veng (85 percent) and those in Kampong Chhnang and Kampong Speu (79 percent in both) were most likely to use antibiotic drugs to treat fever.”
We note that Cambodia is a place where artimisinin resistance has been suspected and yet these DHS results do not diagnose malaria with RDTs as is done in other DHS and MIS surveys. Therefore, appropriate treatment cannot be ascertained from the results. This is made more complicated by the following list of appropriate and inappropriate medicines in the survey instrument that were lumped together under the title “antimalarials”: SP/FANSIDAR, CHLOROQUINE, QUININE, MALARINE, A+M, MEFLOQUINE, ARTEMISININ, ARTESUNATE TABLET, ARTESUNATE SUPPOSITORY, ARTEKINE, COTEXIN.
While the report mentions…
“Iron and folic acid supplementation and antimalarial prophylaxis for pregnant women, promotion of the use of insecticide-treated bednets by pregnant women and children under 5, and six-month deworming for children are some important measures used to reduce anemia revalence among vulnerable groups…”
… it does not report on bednet use.
RBM partners are trying to take the problem of malaria in Asia seriously. They would be assisted by better data on the malaria situation in countries like Cambodia.