Elimination &Eradication Bill Brieger | 16 Jun 2014
Guinea Worm, Inching Toward Eradication
Twenty-eight years ago efforts to eradicate guinea worm began in earnest. It was the UN Water Decade, and there was optimism that guinea worm could be the test case for success of the global effort to guarantee adequate and safe water for all.
 As can be seen in the CDC infographic, we have gone from 3.5 million cases to 148 during this time. As we reach toward the tail end of the worm, we find some challenges remain.
As can be seen in the CDC infographic, we have gone from 3.5 million cases to 148 during this time. As we reach toward the tail end of the worm, we find some challenges remain.
On the list of currently endemic countries one finds Chad. Chad was supposed to be in the pre-certification phase, but new cases appeared a few years ago.
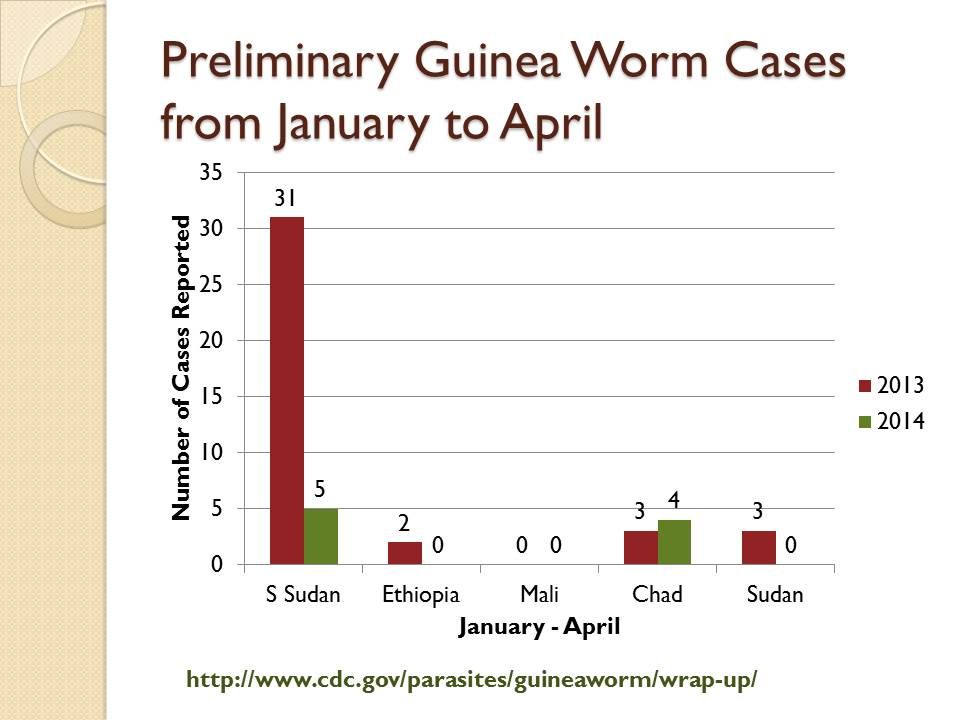
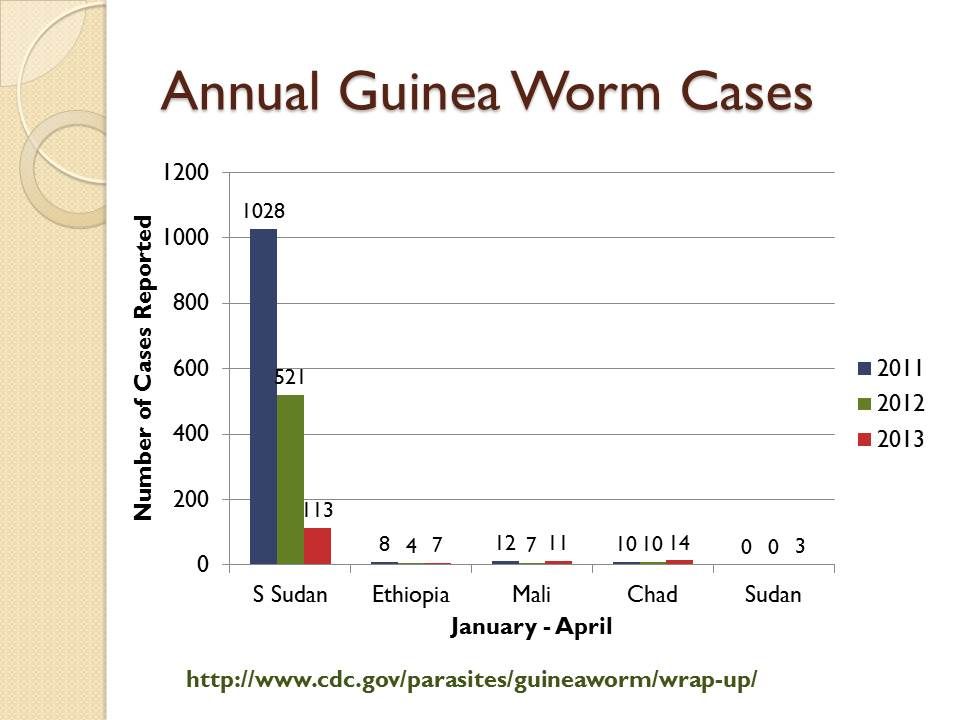 Sudan was the most highly endemic country until South Sudan gained independence and took the guinea worm cases with it. Recently a few cases have also appeared again in the Sudan itself seen in charts derived from CDC’s newsletter, Guinea Worm Wrap-Up.
Sudan was the most highly endemic country until South Sudan gained independence and took the guinea worm cases with it. Recently a few cases have also appeared again in the Sudan itself seen in charts derived from CDC’s newsletter, Guinea Worm Wrap-Up.
Looking at the most recent data from early 2014, one can see that Mali is back to reporting no cases as have Ethiopia and Sudan for 2014. Caution is needed since transmission is more likely in the upcoming rainy season months than in the current dry period.
 What is common in these areas is either being in a state of conflict or bordering a conflict zone. This makes efforts to detect cases and put interventions in place in a timely manner to prevent the next season’s transmission very difficult.
What is common in these areas is either being in a state of conflict or bordering a conflict zone. This makes efforts to detect cases and put interventions in place in a timely manner to prevent the next season’s transmission very difficult.
Unlike some other diseases, guinea worm has some relatively simple, epidemiologically appropriate and less expensive interventions like cloth water filters, abate/temephos for water source treatment and case containment. Of course investments in improved water supplies will also solve the problem. But without easy access to the communities where transmission is occurring, the disease will persist at this incredibly low level.
Other disease elimination programs are equally affected by the problems of access and conflict, polio being a good example. We know that malaria is also exacerbated in conflict situations, but in the locations where pre-elimination is near, like Swaziland, Botswana, South Africa and Namibia, the main concern is ensuring a strong health system to handle the additional surveillance tasks. Still we should not be complacent, because malaria is also endemic in these very sites where guinea worm stubbornly lingers.
Eradication &Health Systems Bill Brieger | 21 Dec 2013
Remembering a Pioneer in International Health and Health Systems: Tim Baker
Honoring people in their lifetime is important, and fortunately Prof. Timothy Baker and his wife Prof Sue Baker were jointly recognized for their many years of service, not only to the Johns Hopkins University Bloomberg School of Public Health, but generally to the fields of global health systems and management. A portrait of the couple was presented and hangs at the School to remind all of their contributions. Unfortunately Tim Baker left us earlier this week.
 While such departures are not often surprising when people have passed their three score and ten, Tim Baker at 88 was still active in teaching, research and service. In fact we served together on the School’s MPH Admissions Committee where Tim Baker brought his wealth of experience and compassion for training students to bear at each meeting. From the student’s point of view, I can saw that even though Tim Baker was not my adviser in during my DrPH at JHU (1989-91), he always looked after my academic progress and was the one to nominate me for Delta Omega (Public Health Honor Society) membership.
While such departures are not often surprising when people have passed their three score and ten, Tim Baker at 88 was still active in teaching, research and service. In fact we served together on the School’s MPH Admissions Committee where Tim Baker brought his wealth of experience and compassion for training students to bear at each meeting. From the student’s point of view, I can saw that even though Tim Baker was not my adviser in during my DrPH at JHU (1989-91), he always looked after my academic progress and was the one to nominate me for Delta Omega (Public Health Honor Society) membership.
On the occasion of the portrait unveiling in 2011, the school shared these brief notes on Dr. Baker’s career: “
Timothy Baker, MD, MPH, a professor in International Health, joined the School as a faculty member in the Department of Public Health Administration and as an assistant dean. In 1961, he founded the School’s Division of International Health and served as acting director. Over the next five years, he was instrumental in building the Division into the Department of International Health. Baker’s fundamental contributions to the Department include faculty recruitment, curriculum development, student mentoring and fundraising. He was instrumental in establishing one of the School’s first endowed professorships—the Edgar Berman Professorship in International Health.
“In more than 50 years as a researcher and consultant, Baker—who holds joint appointments in Health Policy and Management and Environmental Health Sciences—worked in over 40 countries, focusing on health services and assessment of disease and injury burden. He also held leadership positions in several international public health agencies.”
Dr Baker touched many lives. Prof. Peter Winch, Director of International Health’s Social and Behavioral Interventions Program expressed the following in his e-mail to colleagues:
Tim Baker passed away today at the age of 88. I first met him in 1987 as an MPH student when he lectured in Introduction to International Health. It is truly impossible to summarize all of his contributions to the Department of International Health, and to the field of Global Health. This is a quick of superficial overview of his contributions. It is always difficult to know who originated any given idea. But if Tim was not the first one to push the elevator button, he was definitely at the ground floor before the elevator went up. So here is my partial list of his conceptual contributions. This is my paraphrasing of his thinking. He usually expressed such ideas in a more circuitous manner, or did not make a statement at all but rather demonstrated the idea through his actions.
- Public health professionals from low and middle-income countries need training not only on disease prevention and control, but also the design of health systems, management and supervision, leadership and advocacy.
- A central task of global health spending by the US government in low and middle-income countries needs to be capacity-building of local institutions and health professionals. If we don’t do good capacity building, the investments will not yield any lasting results.
- Health systems in low and middle-income countries need to address not only infectious causes of morbidity and mortality, but also occupational health, environmental health, injuries and chronic disease.
- Health workforce development is a complex matter, and warrants high-quality planning, evaluation and research.
- Our School of Public Health benefits from a dynamic, multi-disciplinary, problem-based Department of International Health. Such a Department is an asset to other more disciplinary departments, rather than a threat or a problem.
- Finally: There are no problem students. Every student is an asset. If the faculty identify a student as a problem, there is a good chance the problem lies with the faculty.
Likewise Prof. Adnan Hyder, Director of the Health Systems Program with which Dr. Baker was most recently associated expressed these thoughts:
It is with great sadness that I email you to announce that our beloved Dr. Tim Baker passed away yesterday. This is an incredible loss for our program, the department, and the school to start; but really the entire global health community. As the founder of our department, he was a powerhouse of knowledge, inquiry, and persistence; as a teacher and mentor he was a giant in the field; and as a proponent of the poor and vulnerable, he hid a warm and glowing heart under his witty exterior. So many of us were fortunate to be his students, colleaugues and friends; and how lucky we were to receive his wisdom, insight and sharp advice. Not a man to appreciate praise, he always cut it short; not one to stand pomp and ceremony he often avoided it; and not one to accept failure he believed in the power of humanity to succeed. We will dearly miss him, his humor, his flowers (for ladies only) and his raisin bread – and always remember that he asked us to work harder, and better than anyone else in the world for the cause of social justice and international health.
Let us make sure we never forget his legacy.
Although tropical diseases per se were not Tim Baker’s primary focus, he was concerned about the health systems implications of control programs. In 1962 as the first global effort to eradicate malaria was underway, Tim Baker made the following observations in the American Journal of Public Health:
Malaria eradication “contributes to our own protection. Malaria can be reintroduced into the United States, as several local epidemics have conclusively proved. Just as in the case of yellow fever, where our shores were not safe from imported epidemics until the disease had been controlled in the major ports throughout the world, so it is with
malaria; the world is not safe from the threat of disastrous epidemics until malaria has been eradicated everywhere.” Dr Baker was well aware of challenges that still face us today when he noted that, “widespread development of insecticide resistance lends overwhelming urgency to the completion of eradication.”
He further explained that, “health workers are presented with the opportunity of developing and proving a new method of attack on disease that has tremendous economic import.” The economic impact of malaria remains today one of the driving forces behind efforts to eliminate the disease.
More recently (2007), Dr Baker demonstrated the importance of maintaining a long term perspective. Concerning India’s efforts at controlling malaria from its first through 10th five-year plan, Dr Baker drew on 50+ years of experience to comment that, “The drop from a million to a thousand deaths underscores the value of the malaria program.” It may be another 50 years until malaria is truly eradicated, but if we keep a critical long term view as exemplified by Dr Baker we will be alert to both the challenges and opportunities to bring malaria to an end.
Elimination &Eradication Bill Brieger | 10 Oct 2013
After Dramatic Decline in Malaria Deaths in Africa, Scientists Plan for Final Eradication
 PRESS RELEASE: Thursday, 10 October 2013 at 12:00pm SAST (GMT+2)
PRESS RELEASE: Thursday, 10 October 2013 at 12:00pm SAST (GMT+2)
After Dramatic Decline in Malaria Deaths in Africa, Scientists Plan for Final Eradication: How to win the Endgame Against an Ancient Foe?
At world’s largest meeting of malaria experts, evidence of elimination work underway at edge of disease distribution; focus now turns to malaria heartlands
DURBAN, SOUTH AFRICA (10 OCTOBER 2013)—With widespread use of insecticide-treated nets, indoor spraying and potent malaria medications credited with dramatically reducing malaria deaths in Africa, experts at a major malaria conference discussed the potential to use this progress as a springboard for achieving eradication of a disease that still kills some 660,000 people each year—most of them young African children.
“For the first time we have achieved very large-scale vector control coverage in Africa, and these interventions have prevented a large number of deaths and greatly reduced the burden of transmission,” said Jo Lines, a malaria expert with the London School of Hygiene & Tropical Medicine who previously led the Vector Control Unit of the World Health Organization’s Global Malaria Program. “So while there is a lot of attention still rightly focused on how we can win the battles of today or next week or next year, we can start turning our attention to the longer-term and think about what is needed to win the war.”
Lines was one of several malaria experts discussing the road to malaria eradication in Africa at the Sixth Multilateral Initiative on Malaria (MIM) Pan-African Malaria Conference—the world’s largest gathering of malaria experts—taking place in Durban, South Africa, 6-11 October 2013. Presentations at MIM, including the symposium Lines chaired on “planning for the endgame in Africa,” highlighted how scientists are transitioning from eradication as a lofty aspiration to one that involves an operational plan on the ground.
For example, researchers from South Africa discussed efforts to develop a web site dense with data on local malaria infections, part of the country’s effort to fight practically case by case to achieve its goal of eliminating malaria from the country by 2018. And researchers from Namibia presented the results from a joint effort to police malaria with neighboring Angola, an example, they said, of the cross-border initiatives that will be needed across Africa to eliminate malaria from the continent. Other researchers offered new approaches to malaria control they believe may be more “sustainable.”
According to an abstract by Chistopher Plowe with the Howard Hughes Medical Institute, vaccines are likely to be essential to malaria elimination, given that vaccines have been part of “nearly all successful” infectious disease eradication efforts and “absent from all unsuccessful campaigns.”
THE ELIMINATION CONUNDRUM: MAKING MALARIA GET OUT AND STAY OUT
Lines said that eliminating malaria in Africa requires confronting a range of confounding questions. For example, he noted that increasing access to things like insecticide treated nets and artemisinin combination therapies (ACTs), while crucial to saving lives and reducing disease transmission, comes at a cost: the more they are used, the faster mosquitoes and parasites are likely develop resistance. Also, he said that while malaria transmission patterns are “changing radically” across Africa, it’s not always clear why.
For example, he said his research has documented that there was a significant decrease in malaria transmission in parts of Tanzania before these areas saw widespread use of insecticide treated nets. Meanwhile, in parts of Uganda and Malawi, he said transmission has remained intense despite aggressive use of bed nets and better access to effective medications.
“We don’t know why these interventions are not working equally well in all places in Africa or why in some areas, like Tanzania, the fight against malaria appears to be aided by some other process,” he said. “We do know that when we look back at areas that have eliminated malaria, like the Southern US and Europe, we see that things like land use change, housing and human behavior played a part—potentially a very large part—in conquering the disease.”
Lines said eliminating malaria in Africa requires a better understanding of the different factors affecting transmission and also more attention to disease surveillance. Such work is crucial, he said, to ensuring that once malaria is eliminated from a particular region, it doesn’t simply re-establish itself when an infected individual migrates from areas where malaria is still common.
“The lesson you want to learn from areas that have eliminated malaria is not just how did you drive it out but how did you keep it out,” he said. He said elimination might ultimately need to involve some way of reducing the capacity of mosquitoes or humans to transmit the parasite.
For example, there is work underway today to develop a vaccine that would interrupt the life-cycle of the malaria parasite by preventing it from passing from humans back to mosquitoes. Other efforts have focused on the potential of genetically modified mosquitoes that are rendered incapable of passing along the parasite.
EYES ON THE PRIZE: ELIMINATION VIA DISEASE SURVEILLANCE
In South Africa, which hopes to eliminate malaria by 2018, tracking the total number of infections, recording where they are occurring and following-up to confirm details such as travel history and symptoms is a cornerstone of the country’s elimination strategy. South Africa’s intensive malaria surveillance program includes a website that is constantly updated and features an outbreak alert system and an automated mapping program that can depict malaria cases down to the local level.
A study by Bridget M. Shandukani with South Africa’s National Department of Health found that this type of meticulous surveillance, while costly and labor-intensive, is essential to finishing off malaria in countries like South Africa that have reduced malaria transmission to relatively low levels. She and her colleagues reported that during the 2012-2013 season, all nine of the districts in South Africa at risk for malaria entered into elimination mode, “reporting local case incidences of less than one case per one thousand population at risk.”
Meanwhile, researchers from Namibia presented a study that highlights the importance of cross-border initiatives for countries targeting elimination. They noted that most of the malaria cases in northern Namibia are “imported from southern Angola.” The study examined the effectiveness of a program—the Trans Kunene Malaria Initiative—that implemented a host of interventions in a 20-square kilometer region on both sides of the Namibia-Angola border.
The interventions included long-lasting insecticide treated bed nets, rapid diagnostic tests, community education and case management. Also, both governments agreed to remove customs duties from malaria “commodities,” including bed nets and chemicals used for indoor spraying programs.
The study, presented at MIM and led by Constance Njovu with the JC Flowers Foundation’s Isdell:Flowers Cross Border Malaria Initiative, noted that both areas targeted achieved a significant reduction in malaria. “These results show that cross-border work is both critical to elimination of malaria and possible despite (involving) different national governments with language and cultural differences,” the scientists reported.
Meanwhile, researchers from the University of Pretoria focused on developing “sustainable” tools for malaria control, which they view as crucial to creating more durable reduction in illness and death and thus a more stable platform from which to pursue malaria eradication.
A study by Leo Braack with the University’s Center for Sustainable Malaria Control (CSMC) investigated night-time mosquito biting behavior outdoors, which, given the effectiveness of bed nets, are where an increasing proportion of malaria infections occur. The study found that most bites happen at or near ground level. Braack and his colleagues concluded that simply wearing mosquito-repellent anklets “holds the potential to lower malaria incidence.”
The CSMC’s Taneshka Kruger along with colleagues at the University’s Institute of Applied Materials sought to address limits to bed nets and indoor spraying as control measures: one has to be sleeping under a bed net to enjoy its protection, they noted, while indoor spraying is costly and raises fears of exposure to toxic chemicals. They found that lining interior doors with a mesh fabric treated with a slow-releasing insecticide was a safe, effective and potentially inexpensive form of long-lasting malaria control.
The Multilateral Initiative on Malaria (MIM) (http://www.mimalaria.org/eng/), launched in Dakar, Senegal in 1997, is an international alliance of organizations and individuals seeking to maximize the impact of scientific research against malaria in Africa to ensure that research findings yield practical health benefits. The MIM conference in Durban follows successful conferences held in Yaoundé, Cameroon, in November 2005, and in Nairobi in October 2009. The MIM Secretariat is currently hosted by the Biotechnology Centre of the University of Yaoundé I/Amsterdam Medical Centre.
Media Contacts:
South Africa
Louis Da Gama: +44-7990810642, ldagama@gmail.com
Jessica Rockwood: +27-793517881, jessicarockwood@verizon.net
Geoffrey So: +27-728367853, gso@rbmny.org
Jennifer Jackson: +27.835987778, jennifer.jackson@mrc.ac.za
Keletso Ratsela: +27.828048883, keletso.ratsela@mrc.ac.za
Senegal: Fara Ndiaye: +221.773328863, fara.ndiaye@speakupafrica.org
France: Michel Aublanc: +33-608719795, michel.aublanc@orange.fr
Switzerland: Pru Smith: +41-227914586, smithp@who.int
United Kingdom: Alex Fullem: +44-7787404884, afullem@path.org
USA: Geoffrey So: +1-3479320820, gso@rbmny.org
Trey Watkins: +1-6466266054, kwatkins@rbmny.org
Follow the conversation on social media! #MIM2013 @MIMConf2013
Eradication &Peace/Conflict &Uncategorized Bill Brieger | 23 Jul 2013
Disease Eradication: Somalia Then and Now
In 1978 the US Centers for Disease Control and Prevention reported that, “As of April 14, 1978, no cases of smallpox have been reported to the World Health Organization (WHO) from anywhere in the world since the last case had onset of rash on October 26, 1977, in Merka town, Somalia. However, a total of 2 years of effective surveillance must elapse before this last endemic area can be confirmed to be smallpox-free.” Thirty-five years later Somalia is linked with difficult efforts to eradicate another disease, polio.
Now unfortunately, “Somalia hadn’t had a case of polio for nearly six years. But in the past few months, the virus has come back,” according to National Public Radio (NPR)Â In fact the 73 cases reported from Somalia so far this year, surpasses the 59 cases reported in the rest of the world. NPR further notes that, “Somalia has the rate of polio vaccination in the world after Equatorial Guinea, according to the World Health Organization.”
Thirty-five years ago, challenges hampering disease eradication were the natural environment. “During October and November surveillance in Somalia has been severely hampered by heavy rains that have made it difficult or impossible to travel by vehicle. Since work has had to be continued on foot, there have been some delays in reporting and incomplete search coverage in certain areas,” CDC reported.
Today it is human conflict, not the weather, that inhibits control. NPR’s report notes that, “The Somali government directs the campaigns, but it doesn’t control or have access to vast swaths of the country. Some of the most recent polio cases have occurred in areas that are considered off limits to vaccination teams.” Conflict in Pakistan in December-January also tried to create off limits areas by killing polio workers.
Because polio is a fecal-oral disease it spreads with people. Not surprisingly, cases are appearing in Somali refugee camps in Kenya. All countries in the region are on alert as extra vaccination efforts will be needed. And as NPR observes, this may draw resources from countries like Nigeria that are very close to eliminating the disease. Ironically the polio virus strain found in Somalia was traced to Nigeria.
 Polio cannot be easily compared with malaria which has a vector, and also an larger arsenal of effective tools – insecticide treated nets, indoor residual spraying, chemo-prevention drugs, rapid diagnostic tests and effective medicines. But the diseases face similar challenges that are more often human than deriving from the natural environment. Human conflict deters malaria control in eastern Democratic Republic of the Congo, in the Central African Republic and in South Sudan.
Polio cannot be easily compared with malaria which has a vector, and also an larger arsenal of effective tools – insecticide treated nets, indoor residual spraying, chemo-prevention drugs, rapid diagnostic tests and effective medicines. But the diseases face similar challenges that are more often human than deriving from the natural environment. Human conflict deters malaria control in eastern Democratic Republic of the Congo, in the Central African Republic and in South Sudan.
Unlike for polio, we are not even close to numbering malaria cases in the dozens, but the as the recent Abuja Summit has shown, we must have the political will to rise above conflict and inefficient health systems and face down these devastating diseases.
(PS – fortunately as we can see in the attached map, malaria is not a pressing problem in Somalia.)
Burden &Coordination &Eradication Bill Brieger | 13 Jul 2013
900 Days Left to Make a Big Difference in Malaria as African Ministers of Health Learn in Abuja
A Breakfast Briefing was given to African Ministers of Health and Foreign Affairs on 13th July 2013 in Abuja, Nigeria to review progress in Africa’s fight against malaria and to announce a new initiative to support 10 high-burden countries as part of the Special African Union Summit on HIV/AIDS, Tuberculosis and Malaria.
 Dr Fatoumata Nafo-Traoré, Executive Director, Roll Back Malaria (RBM) Partnership in her welcome address) acknowledged the high level of commitment of partners and the high level of leadership from endemic countries over the past decade in the fight against malaria resulting on 44 countries seeing a > 50% reduction in malaria cases, but we cannot rest in the face of financial and technical challenges.
Dr Fatoumata Nafo-Traoré, Executive Director, Roll Back Malaria (RBM) Partnership in her welcome address) acknowledged the high level of commitment of partners and the high level of leadership from endemic countries over the past decade in the fight against malaria resulting on 44 countries seeing a > 50% reduction in malaria cases, but we cannot rest in the face of financial and technical challenges.
Dr Mustapha Sidiki Kaloko, the African Union Commission’s Commissioner for Social Affairs in his opening remarks reminded us that external funding has never been guaranteed, and as it is ebbing we need to scale up domestic financial support. The AU will work with all stakeholders to help close the $4b gap and not let gains reverse. In order not to lose momentum innovative domestic funding models are needed.
Joy Phumaphi, Executive Secretary of the African Leaders Malaria Alliance (ALMA) delivered the ALMA Scorecard update. She noted that the scorecard provides a roadmap and pushes countries to demonstrate results. Very positive results in terms of adopting policies that oppose artemisinin monotherapies and promote community case management are the norm now.
 The challenge is the low scores on public sector management and effective use of existing resources. Efficiency gains could deliver up to 40% more services with available money. Continued scorecard success also depends on global attention remaining focused on Africa as post MDG goals are being set.
The challenge is the low scores on public sector management and effective use of existing resources. Efficiency gains could deliver up to 40% more services with available money. Continued scorecard success also depends on global attention remaining focused on Africa as post MDG goals are being set.
Dr Robert Newman, Director of the WHO Global Malaria Programme (WHO-GMP) introduced the new Larval Source Management (LSM) Manual. He told the gathering that the new LSM Manual was a result of advocacy by Nigeria’s Minister for Health. IRS and ITNs have been success stories, but we need to use all available tools in appropriate manners. LSM has a unique niche where one finds discrete, fixed and definable water bodies as opposed to water in multiple diffuse sources like cattle foot prints on a rutted road that come and go over days.
Larvicides are expensive and labor intensive and need regular monitoring. People need to remember that environmental management is another larva control tool. With all vector measures “commodities don’t deliver themselvesâ€, but require commitment and action of people at all levels form the national to the community.
Dr Richard Kamwi, Hon. Minister of Health, Namibia, shared that in the 1990s there were 7,000 malaria deaths in his country annually, but only 4 in 2012. Namibia has a mixed strategy especially in the northern border area, and is close to pre-elimination.
Dr Robert Newman, Director of WHO-GMP gave a presentation on the Malaria Situation Room concept and explained that even though progress has been made and millions of lives saved, there are over 219 million cases of malaria annually and 660,000 deaths/ A disproportionate burden of malaria deaths even now is in African children under five years of age. We have responsibility for these children. This burden is focused on 10 countries which account for 70% of malaria cases in Africa and 56% globally.
The Malaria Situation Room will be a way to collate data on funding, intervention, commodities and results. International partners will continue to support all endemic countries, but malaria elimination will remain elusive unless more coordinated action is aimed at high burden areas.
With only 900 days left before the MDGs reach their target date (end of 2015), we want to anticipate and prevent problems like stock-outs, but wait to hear that there have been no antimalarials in clinics for over a month. We want to be proactive in the face of potential dis-investment to protect 10 years of progress which could be undone in only one malaria transmission season.
 Dr Alexandre Manguale, Hon. Minister of Health, Mozambique noted that his country is one of the ten in the “situation room.†Mozambique has made great progress in case reduction in the south with support from the cross border Lubombo Spatial Development Initiative. The rest of the country poses special challenges with logistics and weather (flooding). Under these circumstances partners need to coordinate and be flexible in response to gaps and bottlenecks. Information gathered and shared through the situation room will make this possible.
Dr Alexandre Manguale, Hon. Minister of Health, Mozambique noted that his country is one of the ten in the “situation room.†Mozambique has made great progress in case reduction in the south with support from the cross border Lubombo Spatial Development Initiative. The rest of the country poses special challenges with logistics and weather (flooding). Under these circumstances partners need to coordinate and be flexible in response to gaps and bottlenecks. Information gathered and shared through the situation room will make this possible.
At this point Dr Newman, Dr Nafo-Traoré and Dr Kaloko officially launched the Malaria Situation Room with a ribbon-cutting. Now the work begins to make this ‘room’ a pro-active place to eliminate malaria.
Elimination &Eradication Bill Brieger | 27 May 2013
certifying elimination of guinea worm – lessons for malaria
The efforts to eliminate guinea worm from Nigeria are coming to a close 28 years after the challenge was taken up at national conference in 1985. At the time there were over 650,000 cases in the country. In just eight years between 1988 and 1995 Nigeria saw a precipitous decline in cases down to 16,374 as seen in the attached map from the Carter Center.
 1995 had been posited as the first target date for global guinea worm eradication (see countdown calendar page below), and while efforts came close to eliminating it in Nigeria, the process dragged on for 14 more years until we reached zero annual reported cases. Now there are only a few countries left. The last verifiable case in Nigeria was November 2008. What is the process of ensuring that guinea worm has been eliminated from Nigeria?
1995 had been posited as the first target date for global guinea worm eradication (see countdown calendar page below), and while efforts came close to eliminating it in Nigeria, the process dragged on for 14 more years until we reached zero annual reported cases. Now there are only a few countries left. The last verifiable case in Nigeria was November 2008. What is the process of ensuring that guinea worm has been eliminated from Nigeria?
A major step over the past few years has been to maintain surveillance since guinea work thrives from neglect. As Steve Dada from This Day reported, “WHO officials say finding and containing the last remaining cases of the disease is the most difficult stage of the eradication process, because cases usually occur in remote, hard-to-reach areas.” The communities were involved, as evidenced from a radio announcement heard in Jos, Plateau State last Saturday in which people were encouraged to keep looking for the disease.Surveillance efforts have even made use of events like national immunization days to seek out information on possible cases.
As reported recently in the Vanguard, “The Federal government is offering a cash reward of N25,000 (~$160) for every report of authentic new guineaworm cases in any part of the country. In 2011, a N10,000 reward was offered for a similar report.” So far no authentic case has been found, but indigenous beliefs about the disease has meant many false positives over the years, accounting for the many rumors reported by the Vanguard. These efforts are part of the program to prepare Nigeria for a visiting team from the World health Organization in June 2013 to certify elimination.
 In preparation for eventual certification of all countries, WHO established in 1995 “an independent International Commission for the Certification of Dracunculiasis Eradication in 1995. The Commission comprises 12 public health experts from all six WHO regions.” WHO explains that, “A country reporting zero cases over a period of 12 consecutive months is believed to have interrupted transmission of dracunculiasis and is classified as being in the pre-certification stage … After at least three years of pre-certification and consistent reporting of zero indigenous cases, a country becomes eligible for certification.”
In preparation for eventual certification of all countries, WHO established in 1995 “an independent International Commission for the Certification of Dracunculiasis Eradication in 1995. The Commission comprises 12 public health experts from all six WHO regions.” WHO explains that, “A country reporting zero cases over a period of 12 consecutive months is believed to have interrupted transmission of dracunculiasis and is classified as being in the pre-certification stage … After at least three years of pre-certification and consistent reporting of zero indigenous cases, a country becomes eligible for certification.”
What does all this mean for malaria? First, even though we are talking about a process in Nigeria that spanned nearly three decades, this is relatively short. The characteristics of guinea worm disease (and even small pox, its predecessor in eradication) make it relatively easy to spot. Few people could confuse a worm emerging from one’s body, as seen in the photo from the Carter Center, with another disease. One does not need a microscope either.
 We have been reminded recently that malaria parasites can even ‘hide’ at submicroscopic levels without causing any symptoms. Even with malaria symptoms there is easy confusion by the public with other diseases. We are certainly nowhere near the point of offering $100 rewards for detection of malaria cases.
We have been reminded recently that malaria parasites can even ‘hide’ at submicroscopic levels without causing any symptoms. Even with malaria symptoms there is easy confusion by the public with other diseases. We are certainly nowhere near the point of offering $100 rewards for detection of malaria cases.
There are a number of other key differences such as a ‘vector’ that stays in the pond for guinea worm, while malaria carrying mosquitoes can fly a few miles. The key lesson therefore, is the need to adapt elimination efforts and timelines to the realities of each disease. So while we will not be giving financial rewards for case detection just yet, we should continue to give recognition to Malaria Champions like President Joyce Banda of Malawi.
Another lesson is the fact that WHO established its guinea worm elimination certification process long before all countries were close to reaching goals. This can help malaria program planners envision the surveillance processes they will need to out in place to eliminate the disease, especially since it will likely be, like guinea worm, hiding in the more remote and poor areas of a country.
Finally we must congratulate Nigeria in its guinea worm elimination success and hope this provides motivation for malaria elimination, too.
Eradication Bill Brieger | 17 Mar 2013
South Africa at the Forefront of Malaria Elimination
South Africa as just hosted the 2013 Africa Nations Cup (AFCON) football finals. At the launching of the United Against Malaria (UAM) campaign in collaboration with Confederation of African Football (CAF), RBM (MAWG), and SARN among other partners, the Minister of Health for South Africa explained his country’s commitment to eliminating malaria. Excerpts from the meeting, kindly provided by Daniso Mbewe, summarize the Minister’s remarks.
 “We are so excited to host 2013 AFCON. We love to have visitors come to our beautiful country. One of the advantages to coming to South Africa for the African Cup is the much reduced risk of getting malaria. We are proud to be among the first African countries to be working on eliminating malaria. There are less than 10,000 cases of malaria a year, and they are in an area that we are monitoring closely. Ten years ago, we couldn’t talk about eliminating malaria on the African continent and be taken seriously. Even 5 years ago, many would have never believed it. Today, we have the data to help us tell this story.
“We are so excited to host 2013 AFCON. We love to have visitors come to our beautiful country. One of the advantages to coming to South Africa for the African Cup is the much reduced risk of getting malaria. We are proud to be among the first African countries to be working on eliminating malaria. There are less than 10,000 cases of malaria a year, and they are in an area that we are monitoring closely. Ten years ago, we couldn’t talk about eliminating malaria on the African continent and be taken seriously. Even 5 years ago, many would have never believed it. Today, we have the data to help us tell this story.
“In recent years, we have learned about how a robust health system, with close monitoring of malaria cases can give us the information we need to correctly diagnose and treat each case of malaria. You can’t believe how important it is to track each case down, and be sure that treatment is successful and complete.
“Here in southern Africa; there are already four leading countries well on their way to malaria elimination including provinces and districts in the remaining E8 countries (Botswana, Namibia, Swaziland and South Africa in tier one, and Zimbabwe, Angola, Zambia and Mozambique in tier two) However, for us to stay on track and for other countries to reach sustained malaria control like we have, it required investments and commitments from all sectors. Then and only then, will the malaria map shrink. ”
Of interest, Dr Pakishe Aaron Motsoaledi, the Minister of Health, was born in Phokwane Village in Limpopo – one of the few regions where malaria remains, though at a steadily diminishing rate. The Ministry’s commitment to eliminating malaria is therefore not surprising. In fact South Africa has shown leadership in the region through participation in two cross-border malaria elimination efforts. This is an example of political will that all countries on the continent need to follow.
Eradication Bill Brieger | 24 Nov 2012
The Tail End of Eradication, an Elusive Goal
We are nowhere near eradicating malaria with hundreds of thousands of cases annually throughout the world. It reappears in Greece, and in subclinical form stymies surveillance efforts in the Solomon Islands. But eventually we will close in on this parasite. What can we learn from eradication efforts of another scourge, polio?
Recently the Express Tribune published an article that provided some shock not only in Pakistan, where the issue was detected, but throughout the polio eradication community. “The Prime Minister’s polio cell, the World Health Organisation (WHO), and the United Nations Children’s Fund (UNICEF) confirmed … a newly-found strain of the polio virus.”
The technical reason for the new stain was explained by the international health agencies: cVDPV cases that cause type 2 poliovirus mutate and attain a form that can cause paralysis after passing through multiple children in environments with substandard sanitation. Fortunately polio associated with vaccines is extremely rare, but a more damning administrative explanation of why this may have happened in Pakistan is “poor routine immunization coverage” that enabled these mutations to occur.
Administrative problems include poor scheduling of the current immunization round during a sacred religious period resulted in four districts not participating, but on top of this was a more pressing problem, “the global shortage of the oral polio vaccines especially as anti-polio campaigns are increasing .” This calls into question the upcoming second round of immunization in December. The problem is persistent since it was reported earlier this year that, “Polio coverage (in Pakistan) remained sub-optimal during the past year in Islamabad, as revealed by an independent evaluation report on the post-polio campaign conducted by the World Health Organization.”
 Four endemic countries remain as seen in the graph, and Pakistan’s performance to date is actually better than some of the others, but the situation is volatile, as is the civil/political situation in the remaining affected countries. Interestingly, another eradication-targeted disease, Guinea Worm, was down to 1058 cases in 2011 and remains in only 4 countries, but this is 17 years after the initial date set for its eradication.
Four endemic countries remain as seen in the graph, and Pakistan’s performance to date is actually better than some of the others, but the situation is volatile, as is the civil/political situation in the remaining affected countries. Interestingly, another eradication-targeted disease, Guinea Worm, was down to 1058 cases in 2011 and remains in only 4 countries, but this is 17 years after the initial date set for its eradication.
Polio and Guinea Worm offer malaria some lessons for the present in countries approaching pre-elimination now and those who will hopefully join them over the next decade (if global funding levels are maintained). One lessons is that surveillance is an active part of current polio eradication efforts, otherwise these reports on progress and its challenges would not be published. But the key lesson is that regardless of the effectiveness of the technical intervention (e.g. a vaccine), deployment of the technical intervention is subject to human, administrative, managerial and social complications.
Polio focuses on a vaccine; malaria has treatment medicines, preventive medicines, insecticide sprays, treated bednets, diagnostic tests, and maybe also one day an effective vaccine. It is not too early to plan on how to coordinate all this into achieving effective disease elimination, nationally, regionally and globally.
Diagnosis &Eradication Bill Brieger | 02 Jun 2012
Reactive Malaria Case Detection – Tools for Elimination
Kelly M. Searle, ScM and her advisor at the Johns Hopkins Bloomberg School of Public Health, William J. Moss, MD MPH share the findings from her masters thesis: “Evaluation of Reactive Case Finding to Target Focal Malaria Transmission in Two Different Settings in Macha, Zambia.” They offer ideas on how we can move toward the challenging target of malaria elimination…
 With malaria elimination in the minds of many, new methods of identifying and treating asymptomatic parasite carriers are being investigated. The current study evaluated reactive case detection as a malaria transmission intervention. Reactive case detection is the result of a malaria case being identified in a clinic by passive case detection, testing and treating that individual and their household contacts, and surrounding neighbors.
With malaria elimination in the minds of many, new methods of identifying and treating asymptomatic parasite carriers are being investigated. The current study evaluated reactive case detection as a malaria transmission intervention. Reactive case detection is the result of a malaria case being identified in a clinic by passive case detection, testing and treating that individual and their household contacts, and surrounding neighbors.
Survey sample data from different areas of Macha, Zambia in 2007 and 2008 were used to determine proportions of malaria infected individuals caught passively and reactively. Simulations were done to extrapolate this data to non-sampled households. Radii surrounding identified positive households (index households) were examined to determine the proportion of positive households in each radius.
In the 2007 transmission setting, screening 500 meters surrounding index households would have identified 89% of all households with an RDT positive resident and 90% of all RDT positive individuals. Screening 1 kilometer surrounding index households would have identified 95% of all households with an RDT positive resident and 94% of all RDT positive individuals (Figure 1). In the 2008 transmission setting, screening 500-meters surrounding index households would have identified 77% of all households with an RDT positive resident and 76% of all RDT positive individuals. Screening 1 kilometer surrounding index households would have identified 89% of all households with an RDT positive resident and 89% of all RDT positive individuals (Figure 2).
 Reactive case detection has the potential to be an effective malaria intervention for populations of both moderate transmission settings and transmission settings transitioning (or that have recently transitioned) from moderate to low. With reactive case detection, a large proportion of malaria-infected individuals are accounted for using screening radius of 500 meters. A greater proportion of total households would have to be screened in the lower transmission setting, likely due to the overall lower numbers of cases existing. For reactive case finding to be most effective, it should be targeted at malaria foci and hotspots where transmission is greater than the overall area.
Reactive case detection has the potential to be an effective malaria intervention for populations of both moderate transmission settings and transmission settings transitioning (or that have recently transitioned) from moderate to low. With reactive case detection, a large proportion of malaria-infected individuals are accounted for using screening radius of 500 meters. A greater proportion of total households would have to be screened in the lower transmission setting, likely due to the overall lower numbers of cases existing. For reactive case finding to be most effective, it should be targeted at malaria foci and hotspots where transmission is greater than the overall area.
Elimination &Eradication &Resistance Bill Brieger | 08 Apr 2012
Scale-up Meets Resistance
News this week from The Lancet confirming suspicions of malaria parasite resistance to artemisinin-based drugs deals a double blow to malaria control efforts coming just a few months after announcements by Global Fund to cancel Round 11 funding. Pressure on malaria drugs is nothing new, especially since the same problem has arisen in the same region of the world for two previous and cheaper mainstays of malaria case management.
In all our hopes for rolling back malaria over the past 14 years, did we tell ourselves that such resistance was this time not inevitable?  Unlike in previous waves of resistance, this time we should have been better prepared with effective anti-vector measures. BUT this assumes that we have met our RBM targets and are happily progressing toward 2015 expecting no more malaria deaths.
We get reports that scale-up and case reduction are occurring, such as a recent newspaper article from Jigawa State in Nigeria, but basically we have not achieved our 2010 scale-up targets – so what will come first – 2015 success or the wave of parasite resistance spreading out from Southeast Asia?
The hopes of the current RBM effort were based on the fact that by 2000 we had 3-4 effective anti-malaria interventions, unlike the reliance on mainly one during the first stab at eradication. Unfortunately the question is still the same as it was in the 1950s-60s – are our health systems strong enough to deliver the goods? More effective interventions that do not reach people will not present a strong bulwark against spreading drug resistance.
 Frustration may mount even more when we realize that all the insecticide treated nets distributed over the prolonged period of campaigns from 2009-2012 will need to be replaced, mostly well before 2015. Our coverage to date has not been adequate, our funding is threatened – what guarantees that we can keep up with adequately containing malaria before the resistant strains of the parasite reach Africa where the bulk of cases and deaths occur?
Frustration may mount even more when we realize that all the insecticide treated nets distributed over the prolonged period of campaigns from 2009-2012 will need to be replaced, mostly well before 2015. Our coverage to date has not been adequate, our funding is threatened – what guarantees that we can keep up with adequately containing malaria before the resistant strains of the parasite reach Africa where the bulk of cases and deaths occur?
Some of our ‘easy’ eradication targets like guinea worm and polio are still flaunting their capacity to harm. These like other previous efforts are at risk from donor fatigue. Malaria, which is more complex than those two diseases, is at even greater risk. The RBM Partnership needs to develop a serious and workable strategy to get well ahead to the resistance wave NOW.