Agriculture &Borders &Ebola &Essential Medicines &Integrated Vector Management &ITNs &Larvicide &Mosquitoes &Schistosomiasis &Severe Malaria &Vaccine &Vector Control Bill Brieger | 15 Jul 2019
The Weekly Tropical Health News 2019-07-13
In the past week more attention was drawn to the apparently never-ending year-long Ebola outbreak in the northeast of the Democratic Republic of the Congo. Regarding other diseases, there is new information on the RTS,S malaria vaccine, river prawns have been found to play a biological control role in schistosomiasis, and an update from the World Health Organization on essential medicines and diagnostics. New malaria vector control technologies are discussed.
Second Largest Ebola Outbreak One Year On
Ronald A. Klain and Daniel Lucey in the Washington Post observed raised concern that, “the disease has since crossed one border (into Uganda) and continues to spread. In the absence of a trajectory toward extinguishing the outbreak, the opposite path — severe escalation — remains possible. The risk of the disease moving into nearby Goma, Congo — a city of 1 million residents with an international airport.”
They added their voices to a growing number of experts who are watching this second biggest Ebola outbreak in history and note that, “As the case count approaches 2,500 with no end in sight, it is time for the WHO to declare the outbreak a public health emergency of international concern — a ‘PHEIC’ — to raise the level of global alarm and signal to nations, particularly the United States, that they must ramp up their response.” They call for three actions: 1) improved security for health workers in the region, 2) stepped up community engagement and 3) extended health care beyond Ebola treatment. The inability to adequately respond to malaria, diarrheal diseases and maternal health not only threated life directly, but also threated community trust, putting health workers’ lives at risk.
Olivia Acland, a freelance journalist based in DRC, reporting for the New Humanitarian describes the insecurity and the recent “wave of militia attacks in the Democratic Republic of Congo’s northeastern Ituri province has left hundreds dead and roughly 300,000 displaced in recent weeks, triggering a new humanitarian crisis in a region.” Specifically, “Ituri, a fertile region rich in gold deposits, has been an epicentre of conflict in Congo for decades. Between 1999 and 2003, around 60,000 people were killed here, as a power struggle between rebel groups escalated into ethnic violence,” related to traditional tensions between Hema cattle herders and Lendu farmers with roots in Belgian colonization.
Updates from the DRC Ministry of Health report on average 11 new Ebola cases per day in the past week. So far over 160,000 people have been vaccinated, and yet the spread continues. The Ministry also describes new protocol contains three vaccinations strategies that can be used depending on the environment in which confirmed cases are found including:
- Classic Ring: The classic strategy of vaccinating contacts of confirmed cases and contact contacts.
- Enlarged ring: It is also possible to vaccinate all inhabitants of houses within 5 meters around the outbreak of a confirmed case.
- Geographical Ring: In an area where team safety can not be guaranteed, they can vaccinate an entire village or neighborhood.
Malaria Vaccines, Essential Drugs and New Vector Control Technologies
Halidou Tinto and colleagues enrolled two age groups of children in a 3-year extension of the RTS,S/AS01 vaccine efficacy trial: 1739 older children (aged 5–7 years) and 1345 younger children (aged 3–5 years). During extension, they reported 66 severe malaria cases. Overall they found that, “severe malaria incidence was low in all groups, with no evidence of rebound in RTS,S/AS01 recipients, despite an increased incidence of clinical malaria in older children who received RTS,S/AS01 compared with the comparator group in Nanoro. No safety signal was identified,” as seen in The Lancet.
WHO has updated the global guidance on medicines and diagnostic tests to address health challenges, prioritize highly effective therapeutics, and improve affordable access. Section 6.5.3 presents antimalarial medicines including curative treatment (14 medicines) for both vivax and falciparum and including tablets and injectables. Prophylaxis includes 6 medicines including those for IPTp and SMC. The latest guidance can be downloaded at WHO.
Paul Krezanoski reports on a new technology to monitor bednet use and tried it out in Ugandan households. As a result. “Remote bednet use monitors can provide novel insights into how bednets are used in practice, helping identify both households at risk of malaria due to poor adherence and also potentially novel targets for improving malaria prevention.
In another novel technological approach to vector control, Humphrey Mazigo and co-researchers tested malaria mosquito control in rice paddy farms using biolarvicide mixed with fertilizer in Tanzanian semi-field experiments. The intervention sections (with biolarvicide) had lowest mean mosquito larvae abundance compared to control block and did not affect the rice production/harvest.
Prawns to the Rescue in Senegal Fighting Schistosomiasis and Poverty
Anne Gulland reported how Christopher M. Hoover et al. discovered how prawns could be the key to fighting poverty and schistosomiasis, a debilitating tropical disease. They found that farming the African river prawn could fight the disease and improve the lives of local people, because the African river prawn is a ‘voracious’ predator of the freshwater snail, which is a carrier of schistosomiasis.
The researchers in Senegal said that, “market analysis in Senegal had shown there was significant interest among restaurant owners and farmers in introducing prawns to the diet.” The prawn could also for the basis of aquaculture in rice paddies and remove the threat of schistosomiasis from the rice workers.
—- Thank you for reading this week’s summary. These weekly abstractings have replaced our occasional mailings on tropical health issues due to fees introduced by those maintaining the listserve website. Also continue to check the Tropical Health Twitter feed, which you can see running on this page.
Asymptomatic &Burden &Dengue &Diagnosis &Ebola &Elimination &Epidemiology &Health Systems &ITNs &MDA &Mosquitoes &NTDs &Schistosomiasis &Schools &Vector Control &Zoonoses Bill Brieger | 30 Jun 2019
The Weekly Tropical Health News 2019-06-29
Below we highlight some of the news we have shared on our Facebook Tropical Health Group page during the past week.
Polio Persists
If all it took to eradicate a disease was a well proven drug, vaccine or technology, we would not be still reporting on polio, measles and guinea worm, to name a few. In the past week Afghanistan reported 2 wild poliovirus type 1 (WPV1) cases, and Pakistan had 3 WPV1 cases. Circulating vaccine-derived poliovirus type 2 (cVDPV2) was reported in Nigeria (1), DRC (4) and Ethiopia (3) from healthy community contacts.
Continued Ebola Challenges
In the seven days from Saturday to Friday (June 28) there were 71 newly confirmed Ebola Cases and 56 deaths reported by the Democratic Republic of Congo’s Ministry of Health. As Ebola cases continue to pile up in the Democratic Republic of the Congo (DRC), with 12 more confirmed Thursday and 7 more Friday, a USAID official said four major donors have jump-started a new strategic plan for coordinating response efforts. To underscore the heavy toll the outbreak has caused, among its 2,284 cases, as noted on the World Health Organization Ebola dashboard today, are 125 infected healthcare workers, including 2 new ones, DRC officials said.
Pacific Standard explained the differences in Ebola outbreaks between DRC today and the West Africa outbreak of 2014-16. On the positive side are new drugs used in organized trials for the current outbreak. The most important factor is safe, effective vaccine that has been tested in 2014-16, but is now a standard intervention in the DRC. While both Liberia and Sierra Leone had health systems and political weaknesses as post-conflict countries, DRC’s North Kivu and Ituri provinces are currently a war zone, effectively so for the past generation. Ebola treatment centers and response teams are being attacked. There are even cultural complications, a refusal to believe that Ebola exists. So even with widespread availability of improved technologies, teams may not be able to reach those in need.
To further complicate matters in the DRC, Doctors Without Borders (MSF) “highlighted ‘unprecedented’ multiple crises in the outbreak region in northeastern DRC. Ebola is coursing through a region that is also seeing the forced migration of thousands of people fleeing regional violence and is dealing with another epidemic. Moussa Ousman, MSF head of mission in the DRC, said, ‘This time we are seeing not only mass displacement due to violence but also a rapidly spreading measles outbreak and an Ebola epidemic that shows no signs of slowing down, all at the same time.’”
NIPAH and Bats
Like Ebola, NIPAH is zoonotic, and also involves bats, but the viruses differ. CDC explains that, “Nipah virus (NiV) is a member of the family Paramyxoviridae, genus Henipavirus. NiV was initially isolated and identified in 1999 during an outbreak of encephalitis and respiratory illness among pig farmers and people with close contact with pigs in Malaysia and Singapore. Its name originated from Sungai Nipah, a village in the Malaysian Peninsula where pig farmers became ill with encephalitis.
A recent human outbreak in southern India has been followed up with a study of local bats. In a report shared by ProMED, out of 36 Pteropus species bats tested for Nipah, 12 (33%) were found to be positive for anti-Nipah bat IgG antibodies. Unlike Ebola there are currently no experimental drugs or vaccines.
Climate Change and Dengue
Climate change is expected to heighten the threat of many neglected tropical diseases, especially arboviral infections. For example, the New York Times reports that increases in the geographical spread of dengue fever. Annually “there are 100 million cases of dengue infections severe enough to cause symptoms, which may include fever, debilitating joint pain and internal bleeding,” and an estimated 10,000 deaths. Dengue is transmitted by Aedes mosquitoes that also spread Zika and chikungunya. A study, published Monday in the journal Nature Microbiology, found that in a warming world there is a strong likelihood for significant expansion of dengue in the southeastern United States, coastal areas of China and Japan, as well as to inland regions of Australia. “Globally, the study estimated that more than two billion additional people could be at risk for dengue in 2080 compared with 2015 under a warming scenario.”
Schistosomiasis – MDA Is Not Enough, and Neither Are Supplementary Interventions
Schistosomiasis is one of the five neglected tropical diseases (NTDs) that are being controlled and potentially eliminated through mass drug administration (MDA) of preventive chemotherapy (PCT), in this case praziquantel. In The Lancet Knopp et al. reported that biannual MDA substantially reduced Schistosomiasis haematobium prevalence and infection intensity but was insufficient to interrupt transmission in Zanzibar. In addition, neither supplementary snail control or behaviour change activities did not significantly boost the effect of MDA. Most MDA programs focus on school aged children, and so other groups in the community who have regular water contact would not be reached. Water and sanitation activities also have limitations. This raises the question about whether control is acceptable for public health, or if there needs to be a broader intervention to reach elimination?
Trachoma on the Way to Elimination
Speaking of elimination, WHO has announced major “sustained progress” on trachoma efforts. “The number of people at risk of trachoma – the world’s leading infectious cause of blindness – has fallen from 1.5 billion in 2002 to just over 142 million in 2019, a reduction of 91%.” Trachoma is another NTD that uses the MDA strategy.
The news about NTDs from Dengue to Schistosomiasis to Trachoma is complicated and demonstrates that putting diseases together in a category does not result in an easy choice of strategies. Do we control or eliminate or simply manage illness? Can our health systems handle the needs for disease elimination? Is the public ready to get on board?
Malaria Updates
And concerning being complicated, malaria this week again shows many facets of challenges ranging from how to recognize and deal with asymptomatic infection to preventing reintroduction of the disease once elimination has been achieved. Several reports this week showed the particular needs for malaria intervention ranging from high burden areas to low transmission verging on elimination to preventing re-introduction in areas declared free from the disease.
In South West, Nigeria Dokunmu et al. studied 535 individuals aged from 6 months were screened during the epidemiological survey evaluating asymptomatic transmission. Parasite prevalence was determined by histidine-rich protein II rapid detection kit (RDT) in healthy individuals. They found that, “malaria parasites were detected by RDT in 204 (38.1%) individuals. Asymptomatic infection was detected in 117 (57.3%) and symptomatic malaria confirmed in 87 individuals (42.6%).
Overall, detectable malaria by RDT was significantly higher in individuals with symptoms (87 of 197/44.2%), than asymptomatic persons (117 of 338/34.6%)., p = 0.02. In a sub-set of 75 isolates, 18(24%) and 14 (18.6%) individuals had Pfmdr1 86Y and 1246Y mutations. Presence of mutations on Pfmdr1 did not differ by group. It would be useful for future study to look at the effect of interventions such as bednet coverage. While Southwest Nigeria is a high burden area, the problem of asymptomatic malaria will become an even bigger challenge as prevalence reduces and elimination is in sight.
Sri Lanka provides a completely different challenge from high burden areas. There has been no local transmission of malaria in Sri Lanka for 6 years following elimination of the disease in 2012. Karunasena et al. report the first case of introduced vivax malaria in the country by diagnosing malaria based on microscopy and rapid diagnostic tests. “The imported vivax malaria case was detected in a foreign migrant followed by a Plasmodium vivax infection in a Sri Lankan national who visited the residence of the former. The link between the two cases was established by tracing the occurrence of events and by demonstrating genetic identity between the parasite isolates. Effective surveillance was conducted, and a prompt response was mounted by the Anti Malaria Campaign. No further transmission occurred as a result.”
Bangladesh has few but focused areas of malaria transmission and hopes to achieve elimination of local transmission by 2030. A particular group for targeting interventions is the population of slash and burn cultivators in the Rangamati District. Respondents in this area had general knowledge about malaria transmission and modes of prevention and treatment was good according to Saha and the other authors. “However, there were some gaps regarding knowledge about specific aspects of malaria transmission and in particular about the increased risk associated with their occupation. Despite a much-reduced incidence of malaria in the study area, the respondents perceived the disease as life-threatening and knew that it needs rapid attention from a health worker. Moreover, the specific services offered by the local community health workers for malaria diagnosis and treatment were highly appreciated. Finally, the use of insecticide-treated mosquito nets (ITN) was considered as important and this intervention was uniformly stated as the main malaria prevention method.”
Kenya offers some lessons about low transmission areas but also areas where transmission may increase due to climate change. A matched case–control study undertaken in the Western Kenya highlands. Essendi et al. recruited clinical malaria cases from health facilities and matched to asymptomatic individuals from the community who served as controls in order to identify epidemiological risk factors for clinical malaria infection in the highlands of Western Kenya.
“A greater percentage of people in the control group without malaria (64.6%) used insecticide-treated bed nets (ITNs) compared to the families of malaria cases (48.3%). Low income was the most important factor associated with higher malaria infections (adj. OR 4.70). Houses with open eaves was an important malaria risk factor (adj OR 1.72).” Other socio-demographic factors were examined. The authors stress the need to use local malaria epidemiology to more effectively targeted use of malaria control measures.
The key lesson arising from the forgoing studies and news is that disease control needs strong global partnerships but also local community investment and adaptation of strategies to community characteristics and culture.
Borders &Diagnosis &Ebola &Elimination &Eradication &Health Systems &Measles &Surveillance &Vaccine &Yaws Bill Brieger | 22 Jun 2019
The Weekly Tropical Health News Update 2019-06-22
For almost 20 years we have been maintaining an email list where current news and articles have been shared with those interested in tropical health and malaria. The listserve host we have been using is changing to a paid model. While there are still some free listserve options, these are cumbersome to produce. Since we are already maintaining this blog, we thought it best to provide a weekly summary of key news events through this medium.
Mapping Plasmodium Vivax
The Malaria Atlas Project has published in The Lancet a global burden of Plasmodium Vivax mapping study. The authors describe the contribution of this study as: “Our study highlights important spatial and temporal patterns in the clinical burden and prevalence of P vivax. Amid substantial progress worldwide, plateauing gains and areas of increased burden signal the potential for challenges that are greater than expected on the road to malaria elimination. These results support global monitoring systems and can inform the optimisation of diagnosis and treatment where P vivax has most impact.”
Ebola Spread from DRC to Uganda
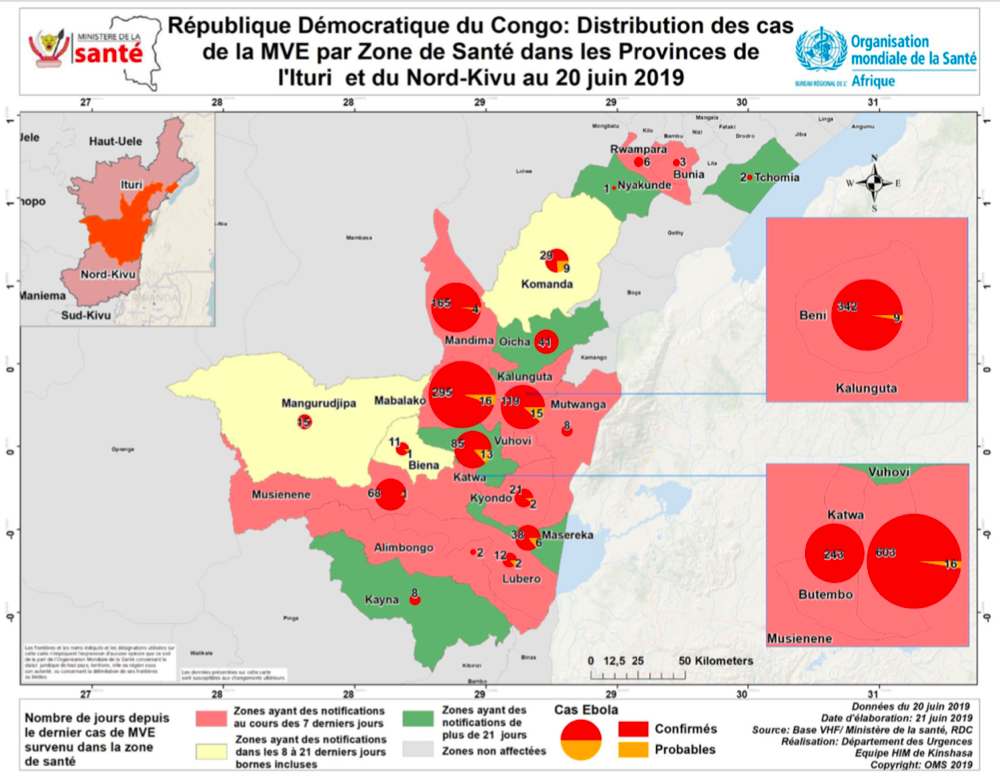 Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation.
Since the major ongoing outbreak of Ebola Virus Disease in North Kivu and Ituri Provinces of the Democratic Republic of Congo (DRC) started nearly a year ago, there has been concern that the disease might spread to neighboring countries like Uganda, Rwanda, South Sudan and the Central African Republic. This fear same true recently when a family affected by Ebola crossed from DRC into Uganda to connect with relatives in Kasese District Uganda. Uganda has had many years’ experience dealing with Ebola and was able to contain the situation.
A press release this week noted that, “As of today (21 June 2019), Uganda has not registered any new confirmed Ebola Virus Disease (EVD) case in Kasese District or any other part of Uganda since the last registered case one week ago. There are no new suspect cases under admission. Currently, 110 contacts to the confirmed Ebola cases in Kagando and Bwera are being followed up daily. A total of 456 individuals have been vaccinated against EVD using the Ebola-rVSV vaccine in Kasese District, Western Uganda.”
Although many people expected that the meeting of the “International Health Regulations (2005) Emergency Committee} for Ebola virus disease in the Democratic Republic of the Congo would finally declare the current outbreak a Public Health Emergency of International Concern (PHEIC) because it crossed a border, the result was noting that the challenge was still an emergency only for DRC. WHO did note that there were serious funding gaps and support from other countries for the DRC’s predicament. Ironically, such gaps make it more likely that Ebola can spread more widely.
As of 21 June 2019, the DRC reported a total of 2,211 cases since the start of the epidemic last year, of which 2,117 have been confirmed and 94 are probable. There have been 1,489 deaths. To date 139,027 persons have been vaccine with the Merck rVSV-ZEBOV vaccine.
Progress toward Eliminating Malaria – the E-2020 Countries
 The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”
The process of eliminating malaria from the world needs to start in a step-by-step fashion. WHO explained that, “Creating a malaria-free world is a bold and important public health and sustainable development goal. It is also the vision of the Global technical strategy for malaria 2016-2030, which calls for the elimination of malaria in at least 10 countries by the year 2020.”
Actually, WHO identified 21 countries, spanning 5 regions, that could defeat malaria by 2020. The progress report charts the effort. During the recent World Health Assembly two countries received recognition for being certified malaria-free, Argentina and Algeria. This week WHO also announced that 5 more countries have not had malaria cases in the past year. There was also release of a downloadable report on progress toward the 2020 target for selected countries.
Reconsidering Yaws Eradication
In the 1950s and 1960s the world focused on the possibility of eradicating Yaws through screening and treatment interventions. Like the early malaria eradication programs from the same period, the Yaws effort slowed, stopped and experienced a resurgence. The Telegraph reported that, “Between 1952 and 1964, Unicef and the WHO screened some 300 million people for the illness, in a coordinated programme which treated more than 50 million cases. Yaws was on the brink of being wiped out and reports of the disease dropped by 95 per cent.” WHO continues to work on treatment strategies with azithromycin and for resistant cases, benzathine benzylpenicillin injection.
WHO noted that there were 80,472 cases reported in 2018, although this figure is likely to be much higher in actuality. The challenge of case detection exists but may be overcome, according to the Telegraph with a new molecular rapid diagnostic test which detects yaws within 30 minutes, and thus could allow on-the-spot diagnosis in remote regions.
Measles Cases Continue to Increase
The problem of measles in the DRC may not be receiving much attention because of the Ebola epidemic. Ironically, Outbreak News Today reports that, “In a follow-up on the measles outbreak in the Democratic Republic of the Congo (DRC), UN health officials report an additional 7500 suspect cases in the past 2 weeks, bringing the total cases since the beginning of the year to 106,870. The death toll due to the measles outbreak has reached 1815 deaths (case fatality ratio 1.7%).”
Vaccine coverage challenges in the DRC result from health systems weaknesses. Unfortunately, a global study has shown that increasing cases in the Global North are not due to weak systems, but ‘vaccine hesitancy.’ The Guardian reports that a global survey has revealed the scale of the crisis of confidence in vaccines in Europe, “showing that only 59% of people in western Europe and 50% in the east think vaccines are safe, compared with 79% worldwide.” The Guardian observes that, “In spite of good healthcare and education systems, in parts of Europe there is low trust in vaccines. France has the highest levels of distrust, at 33%.”
For more news and daily updates check our other services, a closed/private Facebook Group and a Twitter feed. For those who do not use social media, please check here each weekend to find a summary of some of the stories we have shared during the week.
Ebola &Infection Prevention Bill Brieger | 30 Oct 2018
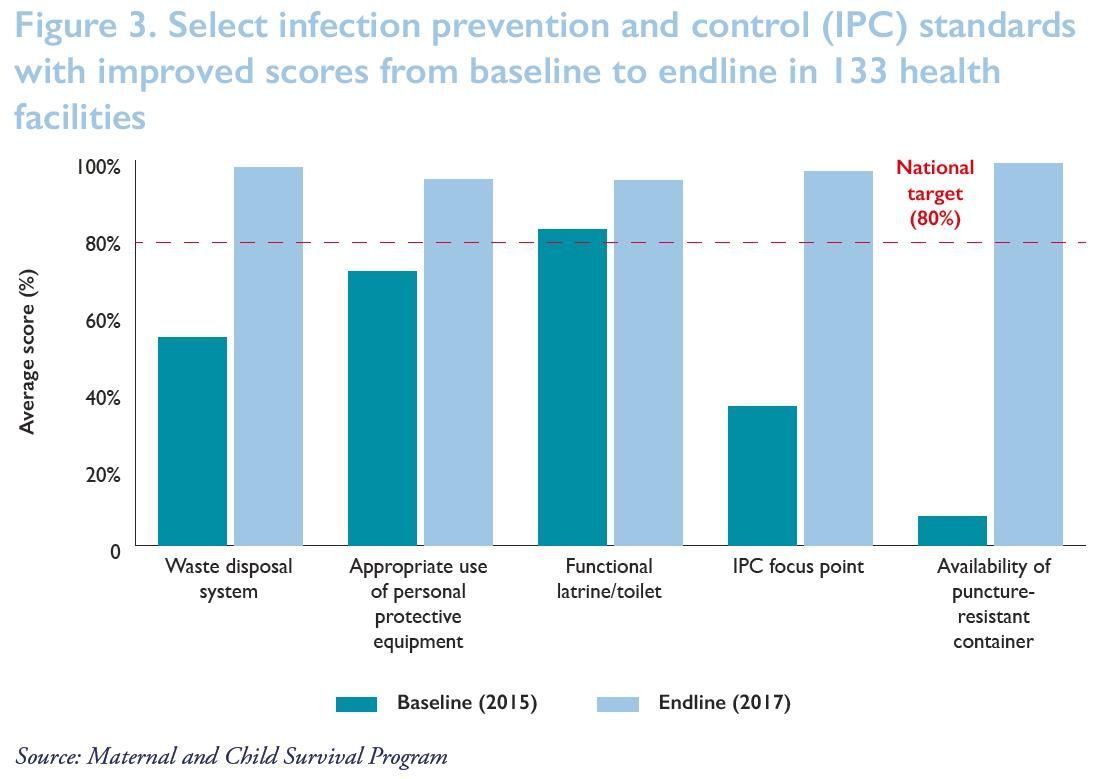
Institutionalizing Infection Prevention and Control: Post-Ebola Experience in Liberian Health Facilities
 Allyson R. Nelson, Anne Fiedler,Topian Zikeh, Nancy Moses, Chandrakant Ruparelia, Lolade Oseni, Mantue Reeves, and Birhanu Getahun presented the work of the Maternal and Child Survival Project in preventing infection among health workers during Ebola and other infectious disease outbreaks. Their efforts are shared below.
Allyson R. Nelson, Anne Fiedler,Topian Zikeh, Nancy Moses, Chandrakant Ruparelia, Lolade Oseni, Mantue Reeves, and Birhanu Getahun presented the work of the Maternal and Child Survival Project in preventing infection among health workers during Ebola and other infectious disease outbreaks. Their efforts are shared below.
 Ebola virus disease (EVD) outbreak in 2014–2015 affected an estimated 4% of the Liberian health workforce. 372 health workers contracted EVD, and 184 died. EVD outbreak and transmission between health care workers and clients highlighted critical gaps in health facilities, especially infection prevention (IPC) practices including waste, water, and triage infrastructure.
Ebola virus disease (EVD) outbreak in 2014–2015 affected an estimated 4% of the Liberian health workforce. 372 health workers contracted EVD, and 184 died. EVD outbreak and transmission between health care workers and clients highlighted critical gaps in health facilities, especially infection prevention (IPC) practices including waste, water, and triage infrastructure.
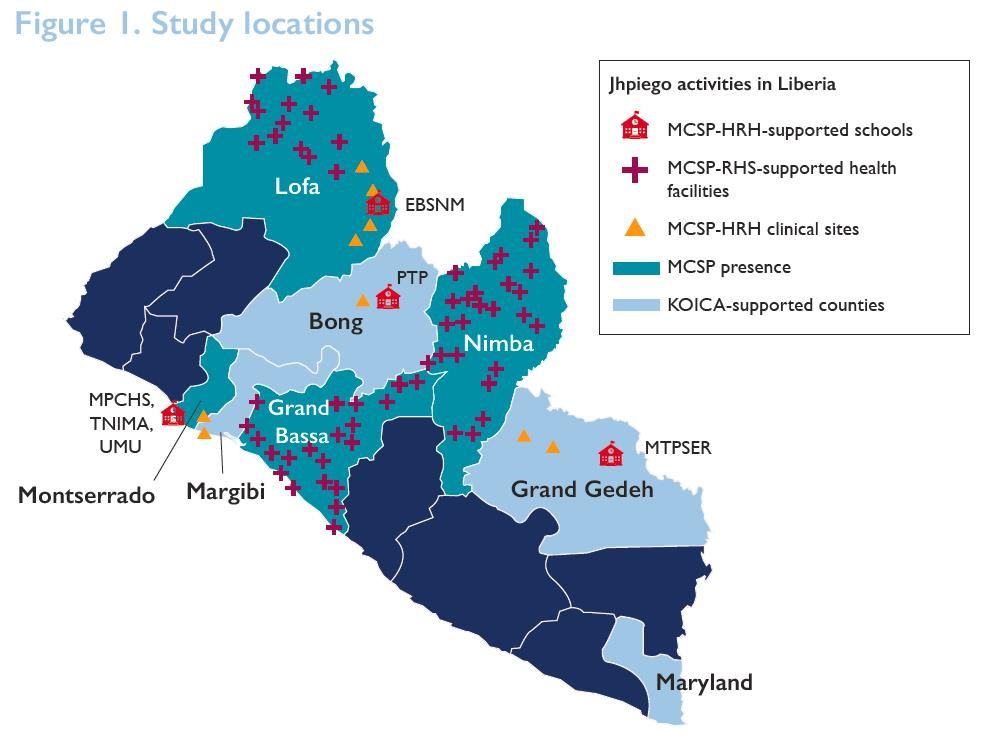
 Liberia’s ministry of health (MOH), with support from Jhpiego and other partners, developed and introduced IPC standards in 2015. Through funding from the Office of U.S. Foreign Disaster Assistance (OFDA), Korea International Cooperation Agency (KOICA), and the United States Agency for International Development’s Maternal and Child Survival Program (MCSP), Jhpiego worked with the MOH to achieve and maintain adherence to IPC standards in over 200 health facilities from 2015 to 2017.
Liberia’s ministry of health (MOH), with support from Jhpiego and other partners, developed and introduced IPC standards in 2015. Through funding from the Office of U.S. Foreign Disaster Assistance (OFDA), Korea International Cooperation Agency (KOICA), and the United States Agency for International Development’s Maternal and Child Survival Program (MCSP), Jhpiego worked with the MOH to achieve and maintain adherence to IPC standards in over 200 health facilities from 2015 to 2017.
 Capacity-building was central to addressing the problem. The team identified critical gaps in skills, infrastructure, supplies hindering adherence to IPC standards. They developed and rolled out standard operating procedures for clinical and nonclinical settings.
Capacity-building was central to addressing the problem. The team identified critical gaps in skills, infrastructure, supplies hindering adherence to IPC standards. They developed and rolled out standard operating procedures for clinical and nonclinical settings.
Partners provided IPC supplies including personal protective equipment (PPE), 90 hand hygiene buckets, Soap, Gloves, 50 waste containers, Rain boots, and Sharps containers.
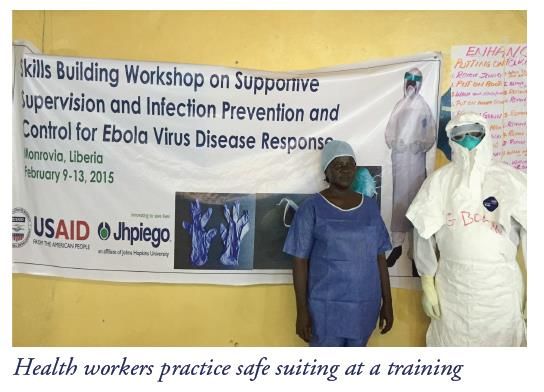 Capacity building included Training (clinical and support personnel). 278 existing health facility staff members as IPC focus points for daily monitoring (OFDA) were trained. Additionally 1,065 health facility staff were trained in Keep Safe Keep Serving IPC and emergency response training (OFDA). Onsite IPC management teams were established in 210 facilities (KOICA and MCSP). Also health workers were offered onsite refresher trainings.
Capacity building included Training (clinical and support personnel). 278 existing health facility staff members as IPC focus points for daily monitoring (OFDA) were trained. Additionally 1,065 health facility staff were trained in Keep Safe Keep Serving IPC and emergency response training (OFDA). Onsite IPC management teams were established in 210 facilities (KOICA and MCSP). Also health workers were offered onsite refresher trainings.
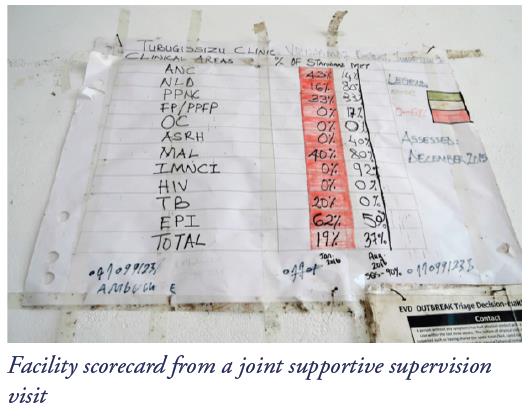 Supportive supervision, mentoring, and coaching were capacity building interventions. 50 district health officers and supervisors were trained in eight counties in supportive supervision, mentoring, and coaching (OFDA). They co-conducted, with district and county health staff, 7,980 weekly and 2,280 monthly supportive supervision visits (OFDA). IPC practices were monitored against the MOH’s IPC minimum standards tool monthly, with scoring, feedback to clinicians and supervisors, and development of action plans for improvement of gaps. Onsite mentoring and coaching was provided on adherence using IPC minimum standards tool at least four times yearly (KOICA and MCSP).
Supportive supervision, mentoring, and coaching were capacity building interventions. 50 district health officers and supervisors were trained in eight counties in supportive supervision, mentoring, and coaching (OFDA). They co-conducted, with district and county health staff, 7,980 weekly and 2,280 monthly supportive supervision visits (OFDA). IPC practices were monitored against the MOH’s IPC minimum standards tool monthly, with scoring, feedback to clinicians and supervisors, and development of action plans for improvement of gaps. Onsite mentoring and coaching was provided on adherence using IPC minimum standards tool at least four times yearly (KOICA and MCSP).
 As a result of the intervention Clinicians and support personnel at program-supported health care facilities adopted, adhered to, and maintained proper IPC practices. This enabled them to provide safe services and evidenced by IPC scores from the Safe, Quality Health Services IPC standards tool. Out of 131 health facilities at endline 99% improved their waste disposal, particularly the availability and use of puncture-resistant sharps containers for the safety of cleaning staff. All (100%) had in place and were using a clear protocol for management and disposal of waste. 98% were segregating waste for safe disposal and management to avoid contamination and spread of infectious disease. 94% had a functional latrine/toilet. All (100%) had operational IPC focus points ensuring adherence to IPC practices. In 95%, staff were regularly using risk-appropriate personal protective equipment during routine care.
As a result of the intervention Clinicians and support personnel at program-supported health care facilities adopted, adhered to, and maintained proper IPC practices. This enabled them to provide safe services and evidenced by IPC scores from the Safe, Quality Health Services IPC standards tool. Out of 131 health facilities at endline 99% improved their waste disposal, particularly the availability and use of puncture-resistant sharps containers for the safety of cleaning staff. All (100%) had in place and were using a clear protocol for management and disposal of waste. 98% were segregating waste for safe disposal and management to avoid contamination and spread of infectious disease. 94% had a functional latrine/toilet. All (100%) had operational IPC focus points ensuring adherence to IPC practices. In 95%, staff were regularly using risk-appropriate personal protective equipment during routine care.
Lessons learned from the intervention showed the importance of the following efforts:
- Comprehensive support is needed to improve adherence to infection prevention and control (IPC) standard practices:
- Capacity-building among health facility staff
- Infrastructure upgrades
- Provision/availability of IPC supplies
- To maintain that adherence after the immediate threat has passed and thus mitigate potential future outbreaks, health facilities need:
- Continuous hands-on mentoring
- Upgraded IPC infrastructure for reproductive, maternal, newborn, child, and adolescent health services
- Changes in behavior and attitudes of health facility staff
- Regular and rigorous data collection and feedback
 This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Abbreviations: EBSNM, Esther Bacon School of Nursing and Midwifery; HRH, Human Resources for Health; KOICA, Korea International Cooperation Agency; MCSP, Maternal and Child Survival Program; MPCHS, Mother Patern College of Health Sciences; MTPSER, Midwifery Training Program-Southeastern Region; PTP, Phebe Paramedical Training Program; RHS, Restoration of Health Services; TNIMA, Tubman National Institute of Medical Arts; UMU, United Methodist University
Announcement &Case Management &CHW &Community &Ebola &Infection Prevention &IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 29 Oct 2018
Malaria Featured in Jhpiego Sessions at ASTMH 2018

Below is a list of Jhpiego Sessions at this week’s American Society of Tropical Medicine Annual Meeting in New Orleans (28 October-1 November). Please attend if you are at the conference:
![]() Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
- Poster Number 098: Performance of community health workers in providing integrated community case management services (iCCM) in 8 districts of Rwanda
- Poster 380: Contribution of quarterly malaria data review and validation to data quality and malaria services Improvement
- Poster LB-5117: Community based health workers can enhance coverage of intermittent preventive treatment of malaria in pregnancy and promote antenatal attendance
Poster Session B, Tuesday 30 October
- Poster 1088: Assessing organizational capacity to deliver quality malaria services in rural Liberia
- Poster 1092: Contribution of IMC project in transforming the face of malaria control for vulnerable populations in Burkina Faso
- Poster 1093: Malaria response plan in times of high transmission: An approach to improving the quality of hospital malaria management
- Poster 1111: Setting the stage to introduce a ground breaking approach to prevent malaria in pregnancy in Sub-Saharan Africa: baseline-readiness assessment findings from Democratic Republic of Congo, Mozambique, Madagascar, and Nigeria
- Poster 1337: Institutionalizing infection prevention and control practices in health facilities in Liberia following the Ebola epidemic
 Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Poster Session C, Wednesday 31 October
- Poster 1816: Experiences and perceptions of care seeking for febrile illness among caregivers and providers in 8 districts of Madagascar
- Poster 1818: Improving adherence to national malaria treatment guidelines by village health workers in selected townships through a low-dose, high-frequency training approach
- Poster 1819: Improving malaria case management through national roll-out of Malaria Service and Data Quality Improvement (MSDQI): A Case study from Tanzania
- Poster 1820: Collaborative quality improvement framework to support data quality improvement, experience from 10 collaborative facilities in Uganda
- Poster 1821: Using malaria death audits to improve malaria case management and prevent future malaria related preventable deaths
- Poster 1833: Multiple approaches for malaria case management in the struggle to reach pre-elimination of malaria.
Scientific Session 182, Thursday, November 1, 10:15 am – 12:00 p.m. Marriott – Balcony I,J,K – 3rd Floor: Seasonal malaria chemoprevention, an effective intervention for reducing malaria morbidity and mortality
Ebola &Hearing Loss &Lassa Fever &Zika Bill Brieger | 03 Mar 2018
World Hearing Day and the Problem of Infectious and Tropical Diseases
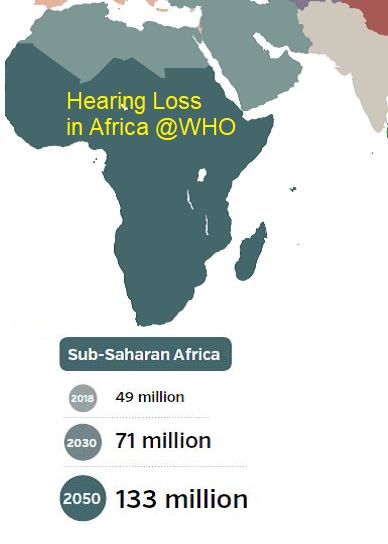
 March 3rd marks the annual World Health Day. The World Health Organization explains that the purpose of this day is to raise awareness on how to prevent deafness and hearing loss and promote ear and hearing care across the world. WHO notes that, “Unless action is taken, by 2030 there will be nearly 630 million people with disabling hearing loss.”
March 3rd marks the annual World Health Day. The World Health Organization explains that the purpose of this day is to raise awareness on how to prevent deafness and hearing loss and promote ear and hearing care across the world. WHO notes that, “Unless action is taken, by 2030 there will be nearly 630 million people with disabling hearing loss.”
Factors associated with health loss and disability include ageing of the population, environmental noise exposure, certain medications, and infectious diseases. It is the latter that we address here.
 Globally there are several infectious diseases associated with hearing loss. In children these include congenital rubella infections a direct result of bacterial meningitis infections, although with improved immunization rates these are less of a problem. In contrast Congenital cytomegalovirus infection has been on the increase.
Globally there are several infectious diseases associated with hearing loss. In children these include congenital rubella infections a direct result of bacterial meningitis infections, although with improved immunization rates these are less of a problem. In contrast Congenital cytomegalovirus infection has been on the increase.
Continuing study of Ebola, Lassa Fever and Zika point to infectious tropical diseases as another serious concern. The large scale of infection and survisorship in Ebola outbreak in West Africa made it possible to study on a large scale reported symptoms of “post-Ebolavirus disease syndrome” (PEVDS) that include, “chronic joint and muscle pain, fatigue, anorexia, hearing loss, blurred vision, headache, sleep disturbances, low mood and short-term memory problems.” A study of 277 Ebola Survivors in one Sierra Leone community found the following clinical sequelae were common: arthralgias (76%), new ocular symptoms (60%), uveitis (18%), and auditory symptoms (24%).
 Lassa Fever has unfortunately made a strong showing in West Africa this dry season. Mateer and colleagues noted an association between Lassa fever (LF) and sudden-onset sensorineural hearing loss (SHNL) was confirmed clinically in 1990. Their literature review found that, “Although LF-induced SNHL has been documented, the prevalence and economic impact in endemic regions may be underestimated.”
Lassa Fever has unfortunately made a strong showing in West Africa this dry season. Mateer and colleagues noted an association between Lassa fever (LF) and sudden-onset sensorineural hearing loss (SHNL) was confirmed clinically in 1990. Their literature review found that, “Although LF-induced SNHL has been documented, the prevalence and economic impact in endemic regions may be underestimated.”
Finally, while much of the focus on the complications of Zika have focused on microcephaly, other problems occur. Zare Mehrjardi et al. documented that Zika Virus may cause “other central nervous system abnormalities such as brain parenchymal atrophy with secondary ventriculomegaly, intracranial calcification, malformations of cortical development (such as polymicrogyria, and lissencephaly-pachygyria), agenesis/hypoplasia of the corpus callosum, cerebellar and brainstem hypoplasia, sensorineural hearing-loss, and ocular abnormalities as well as arthrogryposis in the infected fetuses.”

The benefits of vaccines for rubella and meningitis should spur on immunization research for Ebola, Zika and Lassa Fever. In the meantime there are some preventive measures. One would not have thought that using personal protective equipment by health workers would protect hearing, but it is a practice that should be enabled and encouraged for multiple reasons. Household and community control of Aedes aegypti and rodent breeding to prevent Zika and Lassa, respectively, can also help. By protecting our communities from infection we can also protect their hearing.
Diagnosis &Ebola Bill Brieger | 17 Nov 2016
Mobile suitcase laboratory: A tool for the rapid detection of emerging and endemic infectious disease
Ahmed Abd El Wahed who is based at Georg-August University, Goettingen, Germany shares his experiences with development and use of field diagnostics that can fit in a suitcase. This work received support from the UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases, Geneva, Switzerland. He explains the concept here …
Laboratory diagnosis mainly depends on nucleic acid detection by real-time polymerase chain reaction (PCR), which is available in central laboratories and has a turnaround time of more than two hours. Since real-time RT-PCR assays are not suitable for on-site screening, samples collected from local hospitals, treatment center or at the site of an outbreak have to be sent to laboratories over long distances for testing.
In developing countries, the necessary equipment for diagnosis is only available in few central laboratories, which are not accessible and of limited capacity to test large numbers of incoming samples. Moreover, transport conditions of samples are inadequate and therefore lead to unreliable results.
 For decentralizing of the molecular diagnostics, there is a need for a simple molecular point-of-need test. We have developed a mobile suitcase laboratory (62+49+30 cm) containing all reagents and equipment for the detection of the nucleic acid of infectious agents using the recombinase polymerase amplification (RPA) technology. The RPA assay run at a constant temperature (42°C) for a maximum of 15 minutes.
For decentralizing of the molecular diagnostics, there is a need for a simple molecular point-of-need test. We have developed a mobile suitcase laboratory (62+49+30 cm) containing all reagents and equipment for the detection of the nucleic acid of infectious agents using the recombinase polymerase amplification (RPA) technology. The RPA assay run at a constant temperature (42°C) for a maximum of 15 minutes.
Moreover, all reagents are cold-chain independent and the mobile laboratory is operated by a solar power battery. The nucleic acid extraction is performed by a magnetic bead based method, in which a simple fast lysis protocol is applied. In case of highly infectious agents such as Ebola virus, the inactivation step was performed in a glovebox.
The suitcase lab is designed to detect almost 30 pathogens such as Dengue, Zika, Chikungunya, Ebola, Coronaviruses as well as Tuberculosis, Leptospira, Salmonella typhi and paratyphi, malaria, avian influenza, and Leishmania.
The suitcase lab featured in a presentation at the 65th Annual Meeting of the American Society of Tropical Medicine in Atlanta under the title of “Novel Extraction Protocol and Recombinase Polymerase Amplification Assay for Detection of Leishmania Donovani In 30 Minutes.” Authors/presenters included Dinesh Mondal, Prakash Ghosh, Md. Anik Ashfaq Khan, Faria Hossain, Susanne Böhlken-Fascher, Greg Matlashewski, Axel Kroeger, Piero Olliaro, and Ahmed Abd El Wahed.
Their work highlighted Leishmania donovani (LD), a protozoan parasite transmitted to humans by sand flies, which causes Visceral Leishmaniasis (VL). Currently, diagnosis is based on presence of anti-LD antibodies and clinical symptoms. Molecular diagnosis would require real-time PCR, which is not easy to implement at field settings.
In this study, we report on the development and testing of a novel extraction protocol in combination with recombinase polymerase amplification (RPA) assay for the detection of LD. The LD RPA assay detected equivalent to one LD genomic DNA. The RPA assay was performed at constant temperature (42°C) and the total assay runtime including the extraction procedure was 30 minutes.
The RPA assay also detected other Leishmania species (L. major, L. aethiopica and L. infantum), but did not identify nucleic acid of other pathogens. Forty-eight samples from VL, asymptomatic and post-kala-azar dermal leishmaniasis subjects were detected positive and 48 LD negative samples were negative by both LD RPA and real-time PCR assays, which indicates 100% agreement.
To allow the use of the assay at field settings, a mobile suitcase laboratory (56+45.5+26.5 cm) was developed and operated at the local hospital in Mymensingh, Bangladesh by using a solar-powered battery. DNA extraction was performed by a novel magnetic bead based method, in which a simple fast lysis protocol was applied.
Communication &Ebola Bill Brieger | 07 Nov 2016
Ebola and the Irony of Bush Meat
The deadly Ebola epidemic of 2013-15 in West Africa was suspected of having started when a child in a remote village of Guinea came in contact with infected bats. After that initial episode NONE of the thousands of subsequent cases were traced to zoonotic causes, and yet the health authorities and the media put high level focus on the need to avoid bush meat – whether bats, monkeys, antelope or others – as a prime way to avoid the disease.
 New evidence is emerging that in fact it the evolving relationship between the virus and humans that allowed the disease to spread so widely. within the animal kingdon, humans, not bush meat where the major spreaders of Ebola.
New evidence is emerging that in fact it the evolving relationship between the virus and humans that allowed the disease to spread so widely. within the animal kingdon, humans, not bush meat where the major spreaders of Ebola.
Now two conflicting reports have surfaced about efforts to curb the consumption of bush meat. First, a research team based in Rivers State, Nigeria, one of the places where Ebola reached, conducted a study that tracked the average number of carcases recorded in each market before and after the Ebola virus spread in Nigeria in June 2014. They reported that …
“The markets were surveyed twice a month between March and September 2014. Our survey found a statistically significant fall in trade for all the main traded types of animals. These included antelopes, monkeys, genets, mongooses, rodents, porcupines, birds, crocodiles, turtles and snakes. In particular, the trade in monkeys and fruit bats almost disappeared. Trade in turtles, crocodiles and other cold-blooded species was less affected.”
The group concluded that bush meat, though culturally valued, was “not as important as previously thought for rural people in west Africa.”
 The second report, published a few days later, was posted in the Nigerian newspaper, Vanguard, and echos earlier stories. ”
The second report, published a few days later, was posted in the Nigerian newspaper, Vanguard, and echos earlier stories. ”
“Some bush meat sellers in some major markets in Lagos have said the business is booming again barely two years after the country was declared Ebola Virus Disease free. Some of the bush meat sellers told newsmen on Saturday that they were fully back to their business.”
Behavior change is not a simple process, especially when it comes to culturally rooted practices. Had better hygiene practices been possible by health workers and the public, it is possible that Ebola would have remained isolated. We should worry more about guaranteeing health workers the skills and equipment needed for infection prevention that the sales of bush meat.
Ebola &Infection Prevention &Lassa Fever Bill Brieger | 04 Jun 2016
Poorly Managed Lassa Fever Outbreak in Nigeria
Dr. Obinna O E Oleribe, Chief Executive Officer, E&F Management Care Centre, Abuja Nigeria (Twitter: @OleribeO) shares with readers his view and experiences concerning the August 2015 – May 2016 Lassa Fever outbreak in Nigeria and sees its handling as a strong indicator of weak and failing National Health System.
 On February 6th, 2016, the Vanguard Newspaper reported the growing Lassa Fever outbreak that had killed over 101 persons out of 175 suspected and confirmed cases since August 2015 when the outbreak began in Nigeria. More recently, the World Health Organization (WHO) announced that it had been notified of 273 cases of Lassa fever, including 149 deaths in Nigeria between August 2015 and May 17, 2016. Of the 273, 165 cases and 89 deaths were confirmed through laboratory investigation from 23 states of Nigeria. These deaths include two health care workers out of 10 infected with Lassa fever virus. As at the time of the WHO report (May 17, 2016), eight states were still reporting Lassa fever cases (suspected, probable, and confirmed), deaths and following 248 contacts for the maximum 21-day incubation period.
On February 6th, 2016, the Vanguard Newspaper reported the growing Lassa Fever outbreak that had killed over 101 persons out of 175 suspected and confirmed cases since August 2015 when the outbreak began in Nigeria. More recently, the World Health Organization (WHO) announced that it had been notified of 273 cases of Lassa fever, including 149 deaths in Nigeria between August 2015 and May 17, 2016. Of the 273, 165 cases and 89 deaths were confirmed through laboratory investigation from 23 states of Nigeria. These deaths include two health care workers out of 10 infected with Lassa fever virus. As at the time of the WHO report (May 17, 2016), eight states were still reporting Lassa fever cases (suspected, probable, and confirmed), deaths and following 248 contacts for the maximum 21-day incubation period.
First diagnosed in Nigeria in 1969, Lassa fever (LF) is an acute viral illness caused by Lassa virus, a zoonotic, rodent-borne (multimammate rat), single-stranded ribonucleic acid (RNA) virus from the Arenaviridae, virus family. Since it first isolation in 1969 from a missionary nurse working in Lassa town of Borno State in North-Eastern Nigeria, Lassa Fever has become almost endemic in not only Nigeria, but the West African sub-region as it has continued to be a major public health concern in Nigeria, Liberia, Sierra Leone and Guinea with over 70 million people at risk of the disease. Annually, there are over 3 million cases and about 67,000 deaths from Lassa Fever globally. High association with nosocomial outbreaks, healthcare workers are at increased risk of infection and death. Also, the disease is fast spreading beyond the shores of West Africa into Europe and America from viremic travelers.
A look at the WHO website revealed that Lassa Fever has gained the importance it demanded and was rightly cited on its first page as a disease of public health importance (disease outbreak news). Also, as it is further decreasing the already very limited human resources for health in Nigeria and the rest of West Africa, one would have thought that healthcare managers across the world would have given it the attention it needed.
 In July 2014, Ebola was identified in Nigeria (Lagos State) after Patrick Sawyer imported the disease from Liberia (where there was already an ongoing epidemic). The Lagos State Government, the National Center for Disease Control (NCDC), the Nigerian Field Epidemiology and Laboratory Training Program (NFELTP) and Federal Ministry of Health (FMOH) with the support of well-meaning Nigerian volunteers and some international organizations rose to the occasion and within four months (July 20 – October 20, 2014) kicked Ebola out of Nigeria. They achieved this unbelievable feat through decisive actions, interdisciplinary collaboration, intensive case management, detailed contact tracing, and active port health services. Using isolation, quarantine and supportive management of the infected, case fatality rate was kept at 40% as eight out of the 20 infected individuals succumbed to the virus including several health workers. What was more interesting was the immediate response of government and all relevant stakeholders. The success recorded was to the amazement of the entire world, and completely against all epidemic projects and statistical reasoning.
In July 2014, Ebola was identified in Nigeria (Lagos State) after Patrick Sawyer imported the disease from Liberia (where there was already an ongoing epidemic). The Lagos State Government, the National Center for Disease Control (NCDC), the Nigerian Field Epidemiology and Laboratory Training Program (NFELTP) and Federal Ministry of Health (FMOH) with the support of well-meaning Nigerian volunteers and some international organizations rose to the occasion and within four months (July 20 – October 20, 2014) kicked Ebola out of Nigeria. They achieved this unbelievable feat through decisive actions, interdisciplinary collaboration, intensive case management, detailed contact tracing, and active port health services. Using isolation, quarantine and supportive management of the infected, case fatality rate was kept at 40% as eight out of the 20 infected individuals succumbed to the virus including several health workers. What was more interesting was the immediate response of government and all relevant stakeholders. The success recorded was to the amazement of the entire world, and completely against all epidemic projects and statistical reasoning.
However, few months later, there is another epidemic of another viral hemorrhagic fever. This time around, by a virus that is not as deadly or virulent as Ebola. It has lasted for ten months, killed more people (over 1100% of those killed by Ebola), affected over 800% more cases and with higher case fatality rate of 54%. One, cannot but wonder why Nigeria is finding it difficult to mobilize the same strategies that ended Ebola in Nigeria in 2014 to end Lassa Fever? Or are the structures and personnel not available for this particular outbreak? Or is the will to stop the outbreak lacking among policy makers and healthcare managers?
I believe that there is a need to focus on developing sustainable public health systems that can be mobilized to manage outbreaks across nation; have ready and equipped field workers and foot soldiers who will track, isolate and manage suspected, probable and confirmed cased of any outbreak; and maintain strong surveillance systems able to identify and contain any new, emerging or re-emerging outbreaks.
Nigeria and her leaders should value the lives of the Nigerian people. The government should take health issues more seriously. The citizens of Nigeria need a government that cares. Healthcare workers have a right to live – and not die while working to save other people’s lives. Every hand should be on deck right now to end this outbreak – and as much as possible ensure a delay of its re-emergence.
The time to end Lassa Fever outbreak is NOW. Let us all work towards stopping it once and for all.
Ebola Bill Brieger | 27 Oct 2015
Documenting the Response to the Ebola Epidemic in Liberia through the Perspective of the Local Press
 Join Kwame Sakyi and William R. Brieger of the he Johns Hopkins University at ASTMH Annual Meeting Afternoon Scientific Session #87 on Ebola on Tuesday at 1.45 pm to learn more about how the Liberian Press portrayed Ebola as seen in the Abstract below.
Join Kwame Sakyi and William R. Brieger of the he Johns Hopkins University at ASTMH Annual Meeting Afternoon Scientific Session #87 on Ebola on Tuesday at 1.45 pm to learn more about how the Liberian Press portrayed Ebola as seen in the Abstract below.
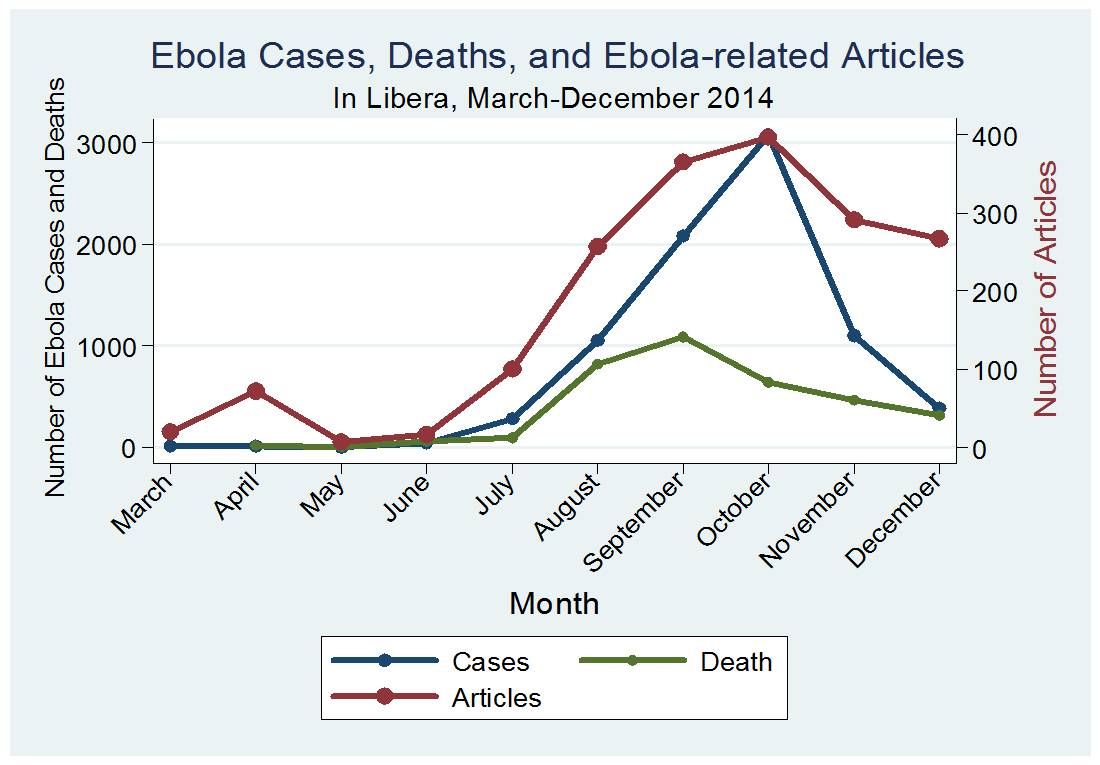
Mass media play an important role in documenting national responses to crises like Ebola. Reviewing media documentation helps a country better prepare for current and future public health challenges. Ebola articles first appeared in the Liberian press in March 2014. Our objectives were to determine the frequency of newspaper accounts and the major issues covered.
We conducted content analysis of Ebola coverage in three Liberian newspapers from March through December 2014. We reviewed electronic publications of three main newspapers by searching for the term “Ebola”.
 Data collected for each article included date of publication, and topic. Data were compiled in Microsoft Excel. After reading the first 50 articles, we inductively generated codes to capture the news content and compiled these into a codebook. The codebook was constantly refined as additional articles were read. Codes were organized into major themes.
Data collected for each article included date of publication, and topic. Data were compiled in Microsoft Excel. After reading the first 50 articles, we inductively generated codes to capture the news content and compiled these into a codebook. The codebook was constantly refined as additional articles were read. Codes were organized into major themes.
A total of 1,793 articles were published across the 3 newspapers over the 10-month period. The frequency of publications on Ebola ranged from 27 in March 2014, but increased to 95 April. Coverage dropped to only 15 in June, but began to rise sharply in August (227), reaching its peak in October (345).
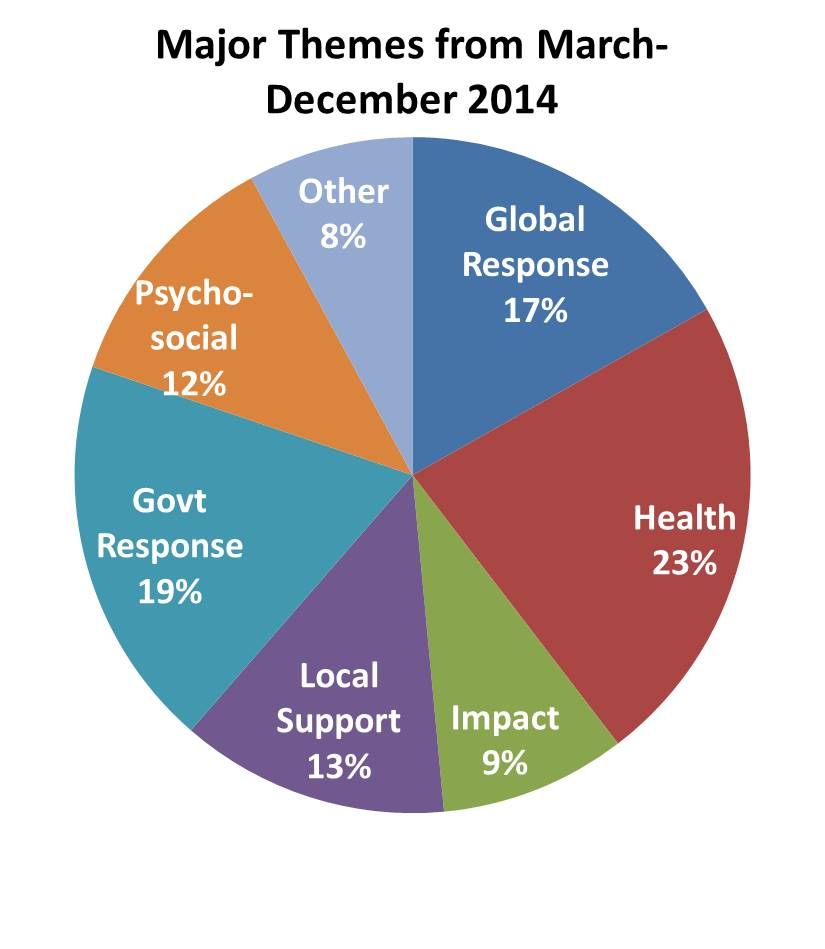 News reports frequency paralleled the incidence pattern of the disease. Major themes included the state of the epidemic, health care, psychosocial issues, international aid, political response, prevention, and local support. Overall political response to Ebola and the impact of Ebola on health workers received the most attention. In the early days common themes were border security and requests for aid.
News reports frequency paralleled the incidence pattern of the disease. Major themes included the state of the epidemic, health care, psychosocial issues, international aid, political response, prevention, and local support. Overall political response to Ebola and the impact of Ebola on health workers received the most attention. In the early days common themes were border security and requests for aid.
At the peak key themes were health worker problems and political responses. A review of the national press during a crisis like Ebola provides a valuable overview of the response of the different players ranging from health services and NGOs to international partners and government. It reflects political will and conflicts and can help a central operations team better coordinate resources and responses of partners.