Case Management &Community &ITNs &Training Bill Brieger | 15 Nov 2017
Community Based Intervention in Malaria Training in Myanmar
 Nu Nu Khin of Jhpiego who is working on the US PMI “Defeat Malaria Project” led by URC shares observations on the workshop being held in Yangon with national and regional/state malaria program staff to plan how to strengthen malaria interventions at the community level. The workshop has adapted Jhpiego’s Community Directed Intervention training package to the local setting.
Nu Nu Khin of Jhpiego who is working on the US PMI “Defeat Malaria Project” led by URC shares observations on the workshop being held in Yangon with national and regional/state malaria program staff to plan how to strengthen malaria interventions at the community level. The workshop has adapted Jhpiego’s Community Directed Intervention training package to the local setting.
 Yesterday’s opening speech was being hailed as a significant milestone to give Community-Based Intervention (CBI) training teams the knowledge, skills, and attitudes they need to effectively provide quality malaria services and quality malaria information.
Yesterday’s opening speech was being hailed as a significant milestone to give Community-Based Intervention (CBI) training teams the knowledge, skills, and attitudes they need to effectively provide quality malaria services and quality malaria information.
 This core team is going to train the critical groups of community-level implementers including CBI focal persons and malaria volunteers at the community level.
This core team is going to train the critical groups of community-level implementers including CBI focal persons and malaria volunteers at the community level.
We embarked this important step yesterday with the collaboration of Johns Hopkins University, Myanmar Ministry of Health and Sports, and World Health Organization Myanmar.
 Participants will be developing action plans to apply the community approach to malaria efforts in townships and villages in three high transmission Rakhine State, Kayin State and Tanintharyi Region.
Participants will be developing action plans to apply the community approach to malaria efforts in townships and villages in three high transmission Rakhine State, Kayin State and Tanintharyi Region.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 08 Nov 2017
Baseline for Coverage of Intermittent Preventive Treatment of Malaria in Pregnancy for Planning Community Interventions in Burkina Faso

Under supervision from health center Community Health Worker provides SP for IPTp to Pregnant Woman
Now that the World Health Organization recommends that pregnant women in high and stable malaria transmission areas receive three or more doses of Intermittent Preventive Treatment (IPTp) with Sulfadoxine-pyrimethamine, it is necessary to learn ways to reach more women with this intervention. William R. Brieger, Mathurin Dodo, Danielle Burke, Ousmane Badolo, Justin Tiendrebeogo, Kristen Vibbert, Susan J Youll, and Julie R Gutman conducted a baseline household survey of recently pregnant women in Burkina Faso to learn about the extent of current IPTp coverage and where improvements are needed. With support from the US President’s Malaria Initiative and the USAID Maternal and Child Survival Program Their findings were made available at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
The World Health Organization recommends intermittent preventive treatment (IPTp) to prevent the adverse effects of malaria in pregnancy in high burden settings; IPTp coverage has lagged behind international targets. In Burkina Faso, the 2014 Malaria Indicator Survey found that 22% of women received 3 or more doses of IPTp (IPTp3). In 2014, Burkina Faso’s IPTp policy was updated from recommending 2 doses to providing at least 3 doses of IPTp. Prior studies have suggested that use of community health workers to deliver IPTp can increase coverage.
 To improve IPTp coverage, we will pilot community delivery of IPTp within 3 southern districts: Po, Ouargaye, and Batie. Here we report results from a baseline assessment in the selected districts. Health Management Information System (HMIS) data for 2015 were collected in each district, and IPTp3 coverage was 37%. Four health facilities per district were randomly selected to participate in the pilot. In 2017, a baseline household survey was conducted among recently pregnant women in the catchment areas of these health facilities.
To improve IPTp coverage, we will pilot community delivery of IPTp within 3 southern districts: Po, Ouargaye, and Batie. Here we report results from a baseline assessment in the selected districts. Health Management Information System (HMIS) data for 2015 were collected in each district, and IPTp3 coverage was 37%. Four health facilities per district were randomly selected to participate in the pilot. In 2017, a baseline household survey was conducted among recently pregnant women in the catchment areas of these health facilities.
 Women were asked to recall the number of antenatal care (ANC) visits and IPTp doses they had received during their most recent pregnancy. The same information was extracted from their ANC cards. A total of 374 women were interviewed during the baseline survey.
Women were asked to recall the number of antenatal care (ANC) visits and IPTp doses they had received during their most recent pregnancy. The same information was extracted from their ANC cards. A total of 374 women were interviewed during the baseline survey.
ANC attendance was reported to be 98% for any visit, and 84% for four visits; these rates were 90% and 62% as documented on the ANC cards. Over 95% of women recalled receiving the first dose of IPTp, while over 80% of cards verified that the first dose was given.
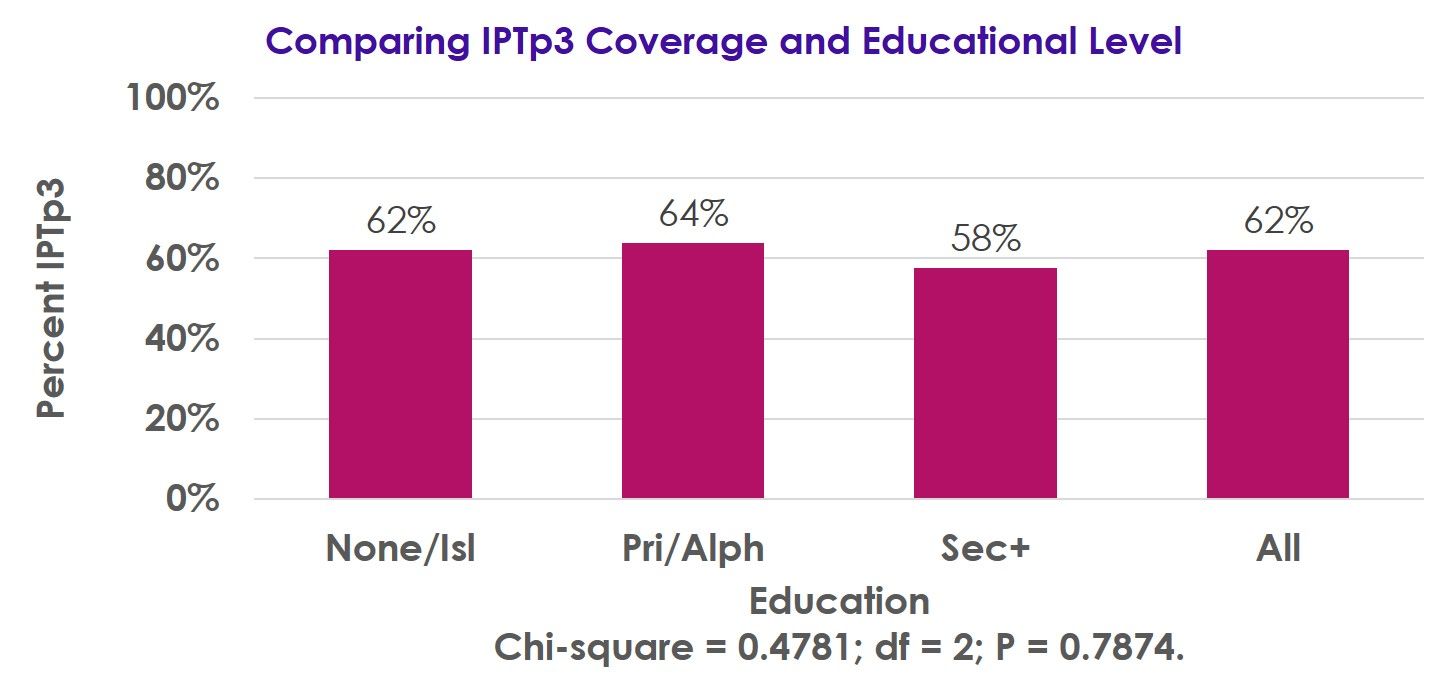 Receipt of the third IPTp dose was 62% by recall and 52% as recorded on the ANC cards, while receipt of 4 doses was 32% by recall and 19% per the ANC cards. IPTp3 coverage was not associated with parity or educational level.
Receipt of the third IPTp dose was 62% by recall and 52% as recorded on the ANC cards, while receipt of 4 doses was 32% by recall and 19% per the ANC cards. IPTp3 coverage was not associated with parity or educational level.
Following implementation of the revised IPTp policy, there has been a substantial improvement in IPTp coverage, though more work is needed to achieve the national 85% coverage target.
Our pilot will examine the impact that delivery of IPTp by community workers has on IPTp coverage, with endline surveys planned for 2018.
CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 07 Nov 2017
Potential Contribution of Community-Based Health Workers to Improving Prevention of Malaria in Pregnancy
 Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Danielle Burke, and Bill Brieger of Jhpiego have designed and are implementing a study to determine the effect of delivering Intermittent Preventive Treatment for Malaria in Pregnancy through community health workers in Burkina Faso with the support of the US President’s Malaria Initiative and the USAID Maternal and Child Survival Project. They have shared the design and start-up activities for the study at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. A summary follows:
Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Danielle Burke, and Bill Brieger of Jhpiego have designed and are implementing a study to determine the effect of delivering Intermittent Preventive Treatment for Malaria in Pregnancy through community health workers in Burkina Faso with the support of the US President’s Malaria Initiative and the USAID Maternal and Child Survival Project. They have shared the design and start-up activities for the study at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. A summary follows:
CHW Flipchart Page
The Ministry of Health of Burkina Faso with the support of its partners initiated a study on the feasibility of increasing provision of Intermittent Preventive Malaria Treatment in pregnant women (IPTp) with sulfadoxine-pyrimethamine (SP) by involving existing community-based health workers (CBHWs). As Burkina Faso adopted the WHO recommendations for more doses of IPTp during pregnancy, it was proposed that the challenge of achieving coverage of third, fourth and additional doses could be met using CBHWs.
The approved protocol calls for CBHWs to refer pregnant women to antenatal care (ANC) to receive their first IPTp dose. Subsequent doses at one-month intervals would be provided by trained CBHWs, who would report back to supervising midwives at the ANC clinics. Several steps were taken to gain approval and set up the intervention.
CHW Using Flipchart
First, IPTp data from the health information system was gathered. IPTp coverage based on ANC registration in the 6 intervention clinics was 69% IPTp1, 68% IPTp2, 56% IPTP3, and 1% IPTp4. Similar information was obtained from the 6 control clinic catchment areas. Situation analysis found that while CBHW curriculum stresses the importance of ANC, it does not address IPTp at community level.
In response updated training materials have been developed. The study team also collected information on village size and availability of CBHWs, especially females. Among the villages in the catchment of the 6 intervention ANC clinics, 33 were found to lack female CBHWs.

Supervisory Meeting
As a result, the team needed to recruit additional female CBHWs, as revised national recruitment guidance stressed attainment of primary school certificate over gender, meaning mainly men had been hired previously. Two institutional review boards were involved and suggested the need to address the potential rare side effects of SP and concerns that community IPTp would not detract from ANC clinic attendance.
Since district and clinic level health staff will be involved in implementing the program using the national CBHW program, lessons learned from this effort to expand the work of CBHWs in preventing malaria in pregnancy should be applicable and adaptable to the whole country.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 21 Oct 2017
Committing to Preventing Malaria in Pregnancy From the National to State to Local Level in Nigeria
Bright Orji recently shared an overview of the Transforming Intermittent Preventive Treatment for Optimal Pregnancy (TIPTOP) Project in Nigeria, a joint venture to protect pregnant women from malaria organized by Jhpiego with support from Unitaid, the National Malaria Elimination Program, The State Ministries of Health in Ebonyi, Niger and Ondo and the local communities. He shares some highlights from the project launch this past week. The project will strengthening antenatal care services to reach out and involve communities in the grassroots delivery of intermittent preventive treatment of malaria in pregnancy (IPTp).

Her Excellency Chief (Mrs.) Rachel Umahi wife Executive Governor Ebonyi State flags off TIPTOP
Among those in attendance were wife of the Ebonyi State Executive Governor and representatives from the State Ministry of Health, the State Malaria Elimination Program, the State Primary Health Care Development Agency, the Ebonyi State House of Assembly, the Ministry of Justice, the Ministry of Local Government, the Ministry of Women Affairs, the School of Nursing and Midwifery, the School of Health Technology Ngbo, the Ohaukwu local government council and the community members.
The media documented the active participation, involvement and commitment by all stakeholders. Other partners present were the World Health Organization representing all UN Agencies in Nigeria and ISGlobal of Barcelona. Furthermore, the villages, families, and traditional rulers of the 16 communities that made up Ohaukwu Communitywelcomed the new project.

In order to emphasize an integrated approach to preventing malaria in pregnancy Ebonyi State, pregnant women given long lasting nets during the TIPTOP launch
Her Excellency Rachel Umahi, wife of the Ebonyi Governor said that, “TIPTOP project came at the right time, and I pledge to join hands to stop malaria in the state.” She was joined by the Ohaukwu Local Government Chairman Barr Clement Oda who shared that, “Today marks a special day in the history of Ohaukwu LGA, Ebonyi State and Nigeria at large as TIPTOP project launch will put the state and her people in the global map. This TIPTOP project will receive a very good support and cooperation from my administration. We shall not relent on what or things we need to do to make this project a success in Ohaukwu LGA worthy for this project.”
The National Coordinator National Malaria Elimination Program, Dr. Bala Audu, explained that, “The choice of Ebonyi state and Ohaukwu LGA in particular is not unconnected with the low utilization of the antenatal care services and low performance in IPTp utilization when compared with other LGAs in the southeastern region. We hope the LGA and the state will use this opportunity to redeem her image in malaria in pregnancy performance in Nigeria.” He pledged his support to Jhpiego and the malaria programs in the three participating states.
Dr. Ugo Okoli, Deputy Country Director Jhpiego in Nigeria pointed out the synergies possible within the state through noting that the, “Maternal and Child Survival Project funded by USAID will collaborate with TIPTOP in Ebonyi State to ensure that ANC is strengthened, and communities mobilized to utilize services.”
Bright Orji will provide updates from time to time in these efforts to reduce the high mortality through community efforts from malaria in pregnancy in Nigeria.
Climate &Community &Development &Epidemiology &Malaria in Pregnancy &Mosquitoes &Surveillance &Urban &Zoonoses Bill Brieger | 11 Jul 2017
Population Health: Malaria, Monkeys and Mosquitoes
 On World Population Day (July 11) one often thinks of family planning. A wider view was proposed by resolution 45/216 of December 1990, of the United Nations General Assembly which encouraged observance of “World Population Day to enhance awareness of population issues, including their relations to the environment and development.”
On World Population Day (July 11) one often thinks of family planning. A wider view was proposed by resolution 45/216 of December 1990, of the United Nations General Assembly which encouraged observance of “World Population Day to enhance awareness of population issues, including their relations to the environment and development.”
A relationship still exists between family planning and malaria via preventing pregnancies in malaria endemic areas where the disease leads to anemia, death, low birth weight and stillbirth. Other population issues such as migration/mobility, border movement, and conflict/displacement influence exposure of populations to malaria, NTDs and their risks. Environmental concerns such as land/forest degradation, occupational exposure, population expansion (even into areas where populations of monkeys, bats or other sources of zoonotic disease transmission live), and climate warming in areas without prior malaria transmission expose more populati ons to mosquitoes and malaria.
ons to mosquitoes and malaria.
Ultimately the goal of eliminating malaria needs a population based focus. The recent WHO malaria elimination strategic guidance encourages examination of factors in defined population units that influence transmission or control.
Today public health advocates are using the term population health more. The University of Wisconsin Department of Population Health Sciences in its blog explained that “Population health is defined as the health outcomes of a group of individuals, including the distribution of such outcomes within the group.” World Population Day is a good time to consider how the transmission or prevention of malaria, or even neglected tropical diseases, is distributed in our countries, and which groups and communities within that population are most vulnerable.
World Population Day has room to consider many issues related to the health of populations whether it be reproductive health, communicable diseases or chronic diseases as well as the services to address these concerns.
CHW &Community &IRS &Treatment Bill Brieger | 27 Apr 2017
Rwanda Celebrates World Malaria Day 2017 – community is a major focus
Dr. Noella Umulisa, the Malaria Team Lead or the USAID Maternal and Child Survival Program in Kigali Rwanda shares with us experiences from Rwanda’s recent observance of World Malaria Day 2017.
The Malaria Day celebration took place in Huye districts in the southern Province. Why the southern province? – because among the 10 high endemic districts, 6 are the southern province. Why Huye district? – because IRS has been launched in Huye district yesterday and in another district Nyanza in Southern province.
 The ceremony was attended by USAID and WHO representative, local leaders, MOH staff, partners, population of Simbi sector and the guest of honour was Dr Jeannine Condo the Director General of Rwanda Biomedical Center (which houses malaria activities).
The ceremony was attended by USAID and WHO representative, local leaders, MOH staff, partners, population of Simbi sector and the guest of honour was Dr Jeannine Condo the Director General of Rwanda Biomedical Center (which houses malaria activities).
A special recognition was given to community health workers (CHWs) who are playing a key role and are on the front line of fighting Malaria through sensitization of the population, testing and treating the population through community case management (iCMM and HBM) of Malaria, and now when a big number of CHWs will be involved in spraying households in their community.
 The World Malaria Day celebration in Rwanda is marked by different activities for Malaria prevention conducted at community level from 24th to 29th April 2017. Also, Malaria prevention and control messages are being disseminated using different communication tools and approaches such as radio and TV programs, community outreach activities, educating communities on proper use of bed nets.
The World Malaria Day celebration in Rwanda is marked by different activities for Malaria prevention conducted at community level from 24th to 29th April 2017. Also, Malaria prevention and control messages are being disseminated using different communication tools and approaches such as radio and TV programs, community outreach activities, educating communities on proper use of bed nets.
Door to door mobilization is being conducted about the Indoor Residual Spraying (IRS) in high malaria burden districts of Huye and Nyanza. MCSP, with support from the US President’s Malaria Initiative, has participated actively in this event by supporting Community outreaches though theatre skits in the first 10 high endemic district.
 The Director General made the following statement:
The Director General made the following statement:
In January 2016, the Government of Rwanda and partners developed a Malaria Contingency Plan in response to the increase in malaria cases. The following interventions were implemented to address malaria rise in Rwanda: A Home Based Management of fever for adults at community level was set up countywide to reduce the malaria burden and prevent severe malaria and death. From Nov 2016 up to March 2017, the country distributed more than 6 million nets in 30 districts ensuring universal coverage of the entire population.
The country has increased access to health services for all through Community Based Health Insurance (CBHI). The Government of Rwanda provides free treatment of malaria to the most vulnerable population (Ubudehe 1&2 categories) to ensure that all financial barriers are no more to hinder the health service delivery for the community. Extension of Indoor residual spraying (IRS) in districts with high malaria burden where 5 out of 8 were sprayed (Nyagatare, Kirehe, Bugesera, Gisagara and Gatsibo).
We hope that this commitment will keep Rwanda on track to control and eventually eliminate malaria.
Community &ITNs &Urban Bill Brieger | 19 Apr 2017
Challenges and Recommendations in Distribution of LLINs in Urban Contexts
by Brooke Farrenkopf

With the malaria team made up of public health nurses and an infectious disease specialist in Kumasi
I participated in a study on urban distribution of long lasting insecticide treated bednets (LLINs) as part of the USAID/PMI VectorWorks Project of the Johns Hopkins University Center for Communication Programs aided by a JHU Global Health Field Placement Scholarship. I conducted qualitative interviews to support a programmatic study on the challenges associated with mass distributions in urban contexts and helped develop report recommendations for developing the guidelines for future campaigns in urban areas. I am sharing my findings here.
As noted VectorWorks is funded by the US President’s Malaria Initiative and works to improve access to long-lasting insecticide treated nets (LLINs) in 12 countries in Asia and Africa. VectorWorks Ghana, through collaboration with the National Malaria Control Program (NMCP) and partners, supports the following distribution campaigns:
- School-based distribution, occurring every May for grades 2 and 6
- Continuous facility-based distribution at ANC and EPI visits
- Point mass distribution campaigns, occurring every 3 years
 In Kumasi, Takoradi, and Tamale, a point mass distribution campaign had already occurred. The campaign in Accra occurred while I was in Ghana, and I was able to visit the distribution sites and the health facilities where a portion of the LLINs were stored. Here, I was able to see some of the logistical challenges associated with the urban context.
In Kumasi, Takoradi, and Tamale, a point mass distribution campaign had already occurred. The campaign in Accra occurred while I was in Ghana, and I was able to visit the distribution sites and the health facilities where a portion of the LLINs were stored. Here, I was able to see some of the logistical challenges associated with the urban context.
I was also able to see the solutions put in place by the local malaria teams. One solution to improve program delivery was the development of a coupon coding system. As each community member attended the distribution site to receive a LLIN, Ghana Health Service (GHS) staff had to match their registration coupon with the coded coupon in the book. The coding system organized the coupons and identified members who had not attended distribution.
Mass distribution campaigns are the most effective method to rapidly increase long-lasting insecticidal net (LLIN) coverage. Mass distribution in urban areas with characteristically large and heterogeneous populations of high population density comes with higher costs and difficult logistics. Many inhabitants are not indigenous to the area and are of varied religious, occupational, and socioeconomic backgrounds. Urban areas commonly have large mobile working class populations that are difficult to access. These characteristics are unique to urban areas and introduces the need for improved guidelines in urban areas.

VectorWorks Ghana Team
To date, the National malaria Control Program (NMCP) guidelines for point mass distribution in Ghana have made no distinction between urban and rural areas and have therefore not addressed these differences. This study intended to provide information to refine these guidelines.
Most interviews were conducted in hospitals and health facilities where the members of the malaria teams were located. The interviews were conducted in-person in the four largest metropolitan areas in Ghana: Kumasi, Greater Accra, Takoradi, and Tamale. I helped develop and follow a question guide that covered each phase of the distribution focusing on the challenges, solutions, and recommendations associated with each phase of distribution.
Most common challenges with implementation in urban communities:
- Reaching community members during registration
- Completing registration within the period of days provided and the volunteers allocated, because the population was too dense to reach all of the households and many community members were not at home during registration
- Beneficiary dissatisfaction with universal health coverage definition of sufficient LLIN coverage {one net per two people in each household}
Most common recommendations for future distributions:
- Greater inclusion of sub-metro teams in development of the micro plan
- Increase the resources to recruit and remunerate more volunteers and supervisors to enable more distribution sites, help control crowds, and allow fewer days for each phase
- Intensify social mobilization and allow sub-metros to help develop this plan to utilize local resources, especially to improve understanding of universal health coverage definition of one net per two people and to inform about logistics
- Increase the number of registration days
- Conduct a utilization study to understand coverage of LLIN use and barriers to consistent use.
I was able to speak with public health nurses, malaria experts, and district health directors, and hear their insight on how to improve future campaigns. My favorite anecdotes included examples of how teams developed innovative solutions to improve campaign efficiency or strategically access hard to reach populations.
The observations and recommendations by the respondents themselves should guide future LLIN campaigns in urban settings in Ghana.
References
- VectorWorks (2017) Johns Hopkins center for Communication Programs. http://ccp.jhu.edu/projects/malaria-vector-control/
- de Beyl CZ, Koenker H, Acosta A, Onyefunafoa EO, Adegbe E, McCartney-Melstad A, Killian A (2016) Multi-country comparison of delivery strategues for mass campaigns to achieve universal coverage with insecticide-treated nets: what works best? Malaria Journal, 15(1): 1.
- Stakeholder Review of Experiences in urban Long-Lasting Insecticidal Net (LLIN) campaign distributions (2012). Malaria Consortium Africa.
CHW &Community Bill Brieger | 12 Apr 2017
Success Stories in Community Health in Africa
 The African Public Health Network of the Johns Hopkins Bloomberg School of Public Health held a panel discussion about community health successes in Africa on Monday 10th of April as the first in a series of events for the annual “Faces of Africa Week”.
The African Public Health Network of the Johns Hopkins Bloomberg School of Public Health held a panel discussion about community health successes in Africa on Monday 10th of April as the first in a series of events for the annual “Faces of Africa Week”.
Africa evokes different reactions to different people. For many, it’s the pictures of starving children, wars, poverty and disease that they find in various print and electronic media. But there has been a lot of achievement in Africa!
The Johns Hopkins Bloomberg School of Public Health – an institution that has invested a lot of time and resources in saving millions of lives at a time- has a huge footprint on the continent and other parts of the developing world through the work done and being done by experienced faculty members. Here is a summary of there thoughts as presented at Monday’s panel.
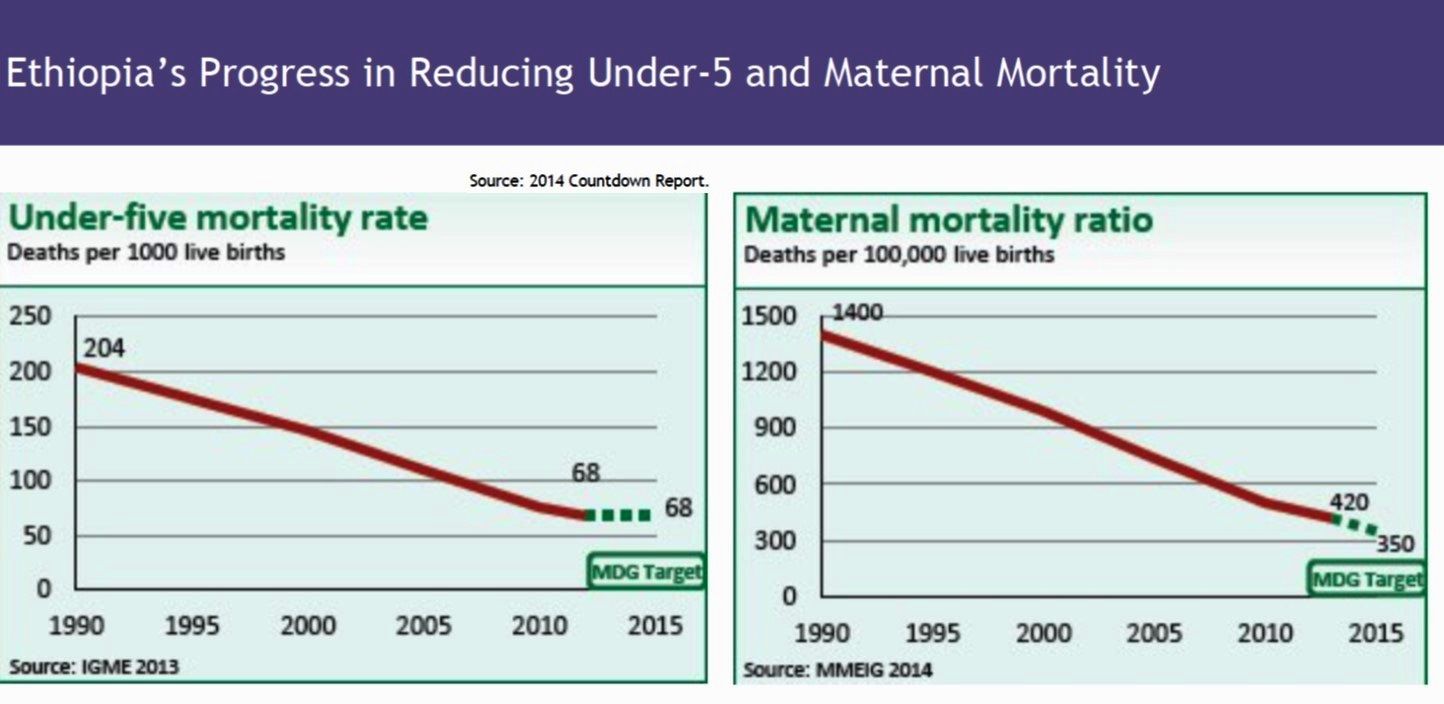 Dr. Henry Perry led the panel discussion on ‘The success stories in Public Health in Africa in the context of the role of Community Based Health Care’. He provided insights from the experiences of Rwanda and Ethiopia. He stressed the achievements of both countries in establishing and scaling up community health worker programs and in achieving Millennium Development Goals with reduced child mortality.
Dr. Henry Perry led the panel discussion on ‘The success stories in Public Health in Africa in the context of the role of Community Based Health Care’. He provided insights from the experiences of Rwanda and Ethiopia. He stressed the achievements of both countries in establishing and scaling up community health worker programs and in achieving Millennium Development Goals with reduced child mortality.
 Dr. William Brieger shared his experience from having lived and worked in Nigeria for over 27 years. He shared the progress in working with volunteer health workers and helping to shape community directed interventions. This history ranged from volunteer CHW programs by local NGOs, FBOs and universities in the 1970s to the development of a standardized set of CHW guidance and training materials by the Federal Ministry of Health in 2012. In the 1990s Nigeria took part in WHO’s African Program for Onchocerciasis Control and established a system of community directed treatment with ivermectin (CDTI) and community directed distributors to enable communities to take charge of annual ivermectin delivery. Then in the 2000s efforts build on the CDTI model to create the community directed intervention approach that included delivery of malaria
Dr. William Brieger shared his experience from having lived and worked in Nigeria for over 27 years. He shared the progress in working with volunteer health workers and helping to shape community directed interventions. This history ranged from volunteer CHW programs by local NGOs, FBOs and universities in the 1970s to the development of a standardized set of CHW guidance and training materials by the Federal Ministry of Health in 2012. In the 1990s Nigeria took part in WHO’s African Program for Onchocerciasis Control and established a system of community directed treatment with ivermectin (CDTI) and community directed distributors to enable communities to take charge of annual ivermectin delivery. Then in the 2000s efforts build on the CDTI model to create the community directed intervention approach that included delivery of malaria  services (ITNs, Case management and intermittent preventive treatment), vitamin A and DOTS for TB through community effort.
services (ITNs, Case management and intermittent preventive treatment), vitamin A and DOTS for TB through community effort.
Dr. Anbrasi Edward shared the Mozambique experience highlighting the Vurhonga projects and the impact of the care group model in improving maternal and child health. She described how the Care Group model was developed by an NGO that involved community volunteers providing education and services to small groups of community members. This model has spread throughout Africa.
 Mr. Bonny Musefano from the Embassy of The Republic of Rwanda provide perspectives on how Rwanda rebuilt its health system after the 1994 genocide ultimately leading to good community health. He stress the importance of Rwanda’s innovative system of community health insurance called Mutuelles de Santé. Very high coverage means that almost all Rwandans have access to health care. He also stressed the country’s interest in innovative technology and how drones are being used to deliver medical supplies to remote areas.
Mr. Bonny Musefano from the Embassy of The Republic of Rwanda provide perspectives on how Rwanda rebuilt its health system after the 1994 genocide ultimately leading to good community health. He stress the importance of Rwanda’s innovative system of community health insurance called Mutuelles de Santé. Very high coverage means that almost all Rwandans have access to health care. He also stressed the country’s interest in innovative technology and how drones are being used to deliver medical supplies to remote areas.
The APHN is grateful to members of the panel and to Prof. David Peters who helped fund the event via the Department of International Health.
For APHN: Joseph Uwazota, Jean Olivier Twahirwa Rwema, Zyleen Kassamali, Eve-Marie Benson, and Massah Massaquoi
Community &Eradication &Malaria in Pregnancy &Women Bill Brieger | 18 Nov 2016
Malaria Mass Drug Administration: Ensuring Safe Care of Reproductive Age Women
The potential impact of mass malaria drug administration (MDA) on pregnant women was the focus of Symposium 146 at the recent 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The symposium was co-chaired by Clara Menéndez and Larry Slutsker who opened the session with an overview.
 As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.
As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.
Current evidence shows that as transmission levels decline, the consequences from P. falciparum malaria are even greater for pregnant women. As countries enter pre-elimination stage and move towards eventual elimination, it will be important to address the needs of pregnant women given their increased vulnerability.
To help achieve elimination, countries are exploring strategies involving widespread distribution of anti-malarials, primarily artemisinin-combination therapies (ACTs), to asymptomatic individuals, including both mass drug administration (MDA) and mass screen and treat (MSaT).
Animal studies have suggested potential embryo toxicity and teratogenic effects of artemisinin drugs in the first trimester of pregnancy.
Given the limited human data, ACTs are currently contraindicated in first trimester, except in documented cases of clinical malaria illness where quinine is unavailable. This poses a challenge in mass campaigns, as it requires the identification of women in early pregnancy who are not yet obviously pregnant. Screening including offering pregnancy tests and/or interview to ask a woman her pregnancy status directly may not work as many may not wish to reveal their pregnancy status.
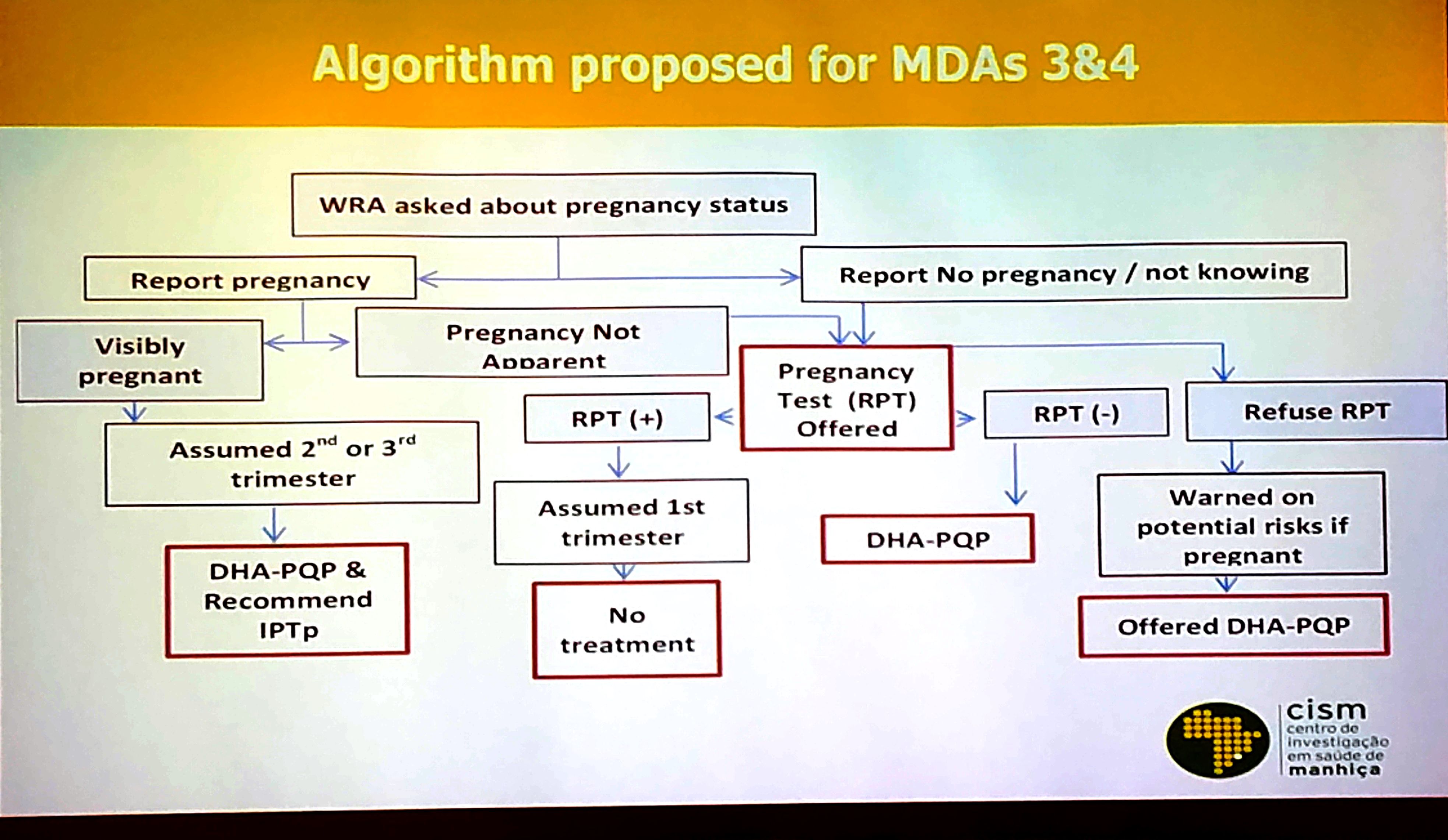
Final Algorithm for Screening Prior to MDA in Mozambique
While only about 5% of the population is pregnant at any given time, and only 1/3 of those are in the first trimester, approximately 20% of the population is comprised of women of reproductive age who may be pregnant. Thus, the number of women who need to be screened for pregnancy is substantial across countries. In addition to privacy issues, costs of screening processes are another barrier.
During the symposium Francisco Saúte from Mozambique and Samuel J. Smith from Sierra Leone shared experiences. Clara Menéndez addressed ethical issues involved in the potential risk of MDA with the ACT Dihydroartemisinin-Piperaquine (DHA-P). These two countries have addressed pregnant women in MDAs in two widely different contexts.
Mozambique is learning whether MDA is a valuable component to malaria elimination in the low transmission areas in the southern part of the country. In Sierra Leone MDA was seen as a lifesaving tool to prevent malaria deaths during the Ebola epidemic when taking blood samples for diagnosis was a major risk.
Over several rounds of MDA, Mozambique refined its pregnancy screening procedures over several rounds of MDA as seen in the attached slide. Costs, confidentiality, convenience and efficiency entered into the equation that saw a greater focus on communicating with women rather that testing. Lessons learned from MDA in Mozambique included –
- Screening for early pregnancy in the context of MDA is challenging, particularly among teenage girls where disclosing pregnancy can be problematic
- Need to train field workers (preferably women) about the need to ensure confidentiality of pregnancy testing/results
- Confidentiality is also crucial to ensure adherence to t

MDA Rationale in Sierra Leone during Ebola Outbreak
he pregnancy testing
- Women not accepting pregnancy test must be warned on risks/ benefits of ACTs in 1st trimester
- Health authorities must understand that IPTp and MDA are not mutually exclusive

The Ebola epidemic in Sierra Leone and its neighbors, Liberia and Guinea, devastated the health workforce, and the availability of any sort of testing supplies was low. The country experienced a major drop in utilization of clinic based MCH services including those for malaria during the period.

MDA Goals in Sierra Leone
Because of initial similarities in presenting symptoms between Ebola and malaria, people were often fearful of going to the health center in case they were detained for Ebola care or were exposed to other patients who had Ebola. Community MDA seemed to be one way to protect the population from malaria in this emergency situation. The attached slide offers a rational for the MDA. A second slide explains Sierra Leone’s goal for MDA with Artesunate-Amodiaquine in the context of Ebola. Though not completely, the Sierra Leone MDAs were able to exclude pregnancy women in their first trimester.

Pregnant women excluded from MDA in Sierra Leone
In conclusion MDA is a tool conceived primarily for countries and areas of countries as part of the pre-elimination strategy. It presents a variety of logistical challenges, but a major concern should also be the ethical issues of giving a potentially toxic drug to women in their first trimester of pregnancy. Alternative strategies to protect these women, including insecticide treated nets, must be explored.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 16 Nov 2016
Gaining an early start to IPTp through promotion of MIP at the community level in Kenya
 A poster entitled “Community health: Improving start of IPTp early in second trimester through promotion of MIP at the community level in Kenya” was presented by Augustine Ngindu, Gathari Ndirangu, E Nyapada, David Omoit, and Mildred Mudany from Jhpiego’s Kenya Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
A poster entitled “Community health: Improving start of IPTp early in second trimester through promotion of MIP at the community level in Kenya” was presented by Augustine Ngindu, Gathari Ndirangu, E Nyapada, David Omoit, and Mildred Mudany from Jhpiego’s Kenya Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
WHO policy recommends that pregnant women living in moderate to high malaria transmission areas start receiving intermittent preventive treatment in pregnancy (IPTp) with sulfadoxine pyrimethamine (SP) early in second trimester to prevent malaria in pregnancy (MIP).

Training Community Health Volunteers in Bungoma
In Bungoma County, Kenya, 52% of pregnant women start IPTp in their third trimester. Between June and September 2015, 197 Community Health Assistants (CHAs) were trained, who in-turn trained 2,344 Community Health Volunteers (CHVs) in Bungoma County.
Following the training, CHVs registered new pregnant women at their homes and encouraged them to seek antenatal care (ANC) and start taking IPTp early in the second trimester. The CHVs also helped to identify previously registered women who were not attending ANC and refer them to ANC for MIP services.
The CHVs, with CHA supervision, reached 44,133 pregnant women with MIP messages on starting IPTp early in the second trimester and use of a net. Data from 70 health facility registers was collected biannually and showed a 12% increase (24%-36%) in the proportion of pregnant women starting ANC attendance ? 20 weeks of pregnancy between October 2014 and March 2016.

Community Health Volunteers Encourage ANC Attendance
Although there was a decline in the proportion of women receiving IPTp-SP between October 2014 and January 2015 and between October 2015 and February 2016 due to SP stock-outs, this did not significantly affect ANC attendance. The 12% increase in early ANC attendance is likely associated with CHV efforts in sensitizing women to start IPTp early in the second trimester and indicates a positive change in health seeking behaviour that can be sustained over time provided the commodities are available.
The success with CHVs promoting MIP at the community level has led to it being replicated in three additional counties and it will be extended in phases in other malaria endemic counties.