CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 29 Oct 2018
Community Health Workers Can Enhance Coverage of Intermittent Preventive Treatment of Malaria in Pregnancy and Promote Antenatal Attendance
Among the poster presentations on malaria from Jhpiego, the President’s Malaria Initiative and partners at the 2018 ASTMH Annual Meeting, WR Brieger, J Tiendrebeogo, O Badolo, M Dodo, D Burke, K Vibbert, SJ Youll, and JR Gutman shared the findings from a 15-month intervention that tested the ability of community health workers to deliver intermittent preventive treatment of malaria in pregnancy in 3 districts in Burkina Faso. Please check out the poster and talk to one of the co-investigators at Poster Session A on Monday 29 October. Their results are found below.
Malaria in pregnancy is responsible for a substantial proportion of low-birthweight and stillborn infants in sub-Saharan Africa. To prevent this, the World Health Organizatio n (WHO) recommends that pregnant women receive intermittent preventive treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine. Specifically, WHO recommends an optimal three or more doses (e.g., IPTp3, IPTp4).
n (WHO) recommends that pregnant women receive intermittent preventive treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine. Specifically, WHO recommends an optimal three or more doses (e.g., IPTp3, IPTp4).
In stable malaria endemic countries, IPTp coverage remains unacceptably low, at around 19% for IPTp3. Community IPTp might provide an answer. Community delivery can improve coverage as seen in previous study in Nigeria and Malawi, but its effects on antenatal care (ANC) attendance have been mixed. Additional data are needed to determine whether delivery of IPTp-SP by community health workers (CHWs) is effective and does not detract from ANC attendance. Hence the Burkina Faso intervention was designed and implemented
The study piloted community delivery of IPTp (c-IPTp) in three districts of Burkina Faso  with high malaria transmission: Po, Ouargaye, and Batie. Four health facilities per district were randomly selected to participate (two intervention and two control).
with high malaria transmission: Po, Ouargaye, and Batie. Four health facilities per district were randomly selected to participate (two intervention and two control).
In 2017, following a baseline household survey of women who recently became pregnant, implementation of c-IPTp began in intervention areas by existing CHWs trained and supervised by health staff. At Baseline in each of the three study districts, four health centers (CSPSs) and the villages in their catchment areas were selected—two as intervention and two as control. A random sample of 374 women who had been pregnant within the last 9 months were interviewed in CSPS catchment villages. There were no significant differences in ANC attendance (ANC1=90%, ANC4=62%) or IPTp coverage between intervention and control areas:
- IPTp3 was 81% (intervention) and 86% (control).
- IPTp4 was 22% (intervention) and 16% (control).
 The Intervention consisted of building on Burkina Faso’s existing CHWs. They were trained and monitored by clinic staff. The CHWs encouraged women to attend the first ANC visit to obtain IPTp1. Then the CHWs provided monthly doses of IPTp, submitted monthly reports, and continued to promote ANC. ANC attendance and IPTp uptake were monitored through monthly clinic and CHW reports. The catchment area populations were roughly the same, and monitoring showed that the additional provision of IPTp by CHWs resulted in more women being reached while at the same time ANC attendance remained high.
The Intervention consisted of building on Burkina Faso’s existing CHWs. They were trained and monitored by clinic staff. The CHWs encouraged women to attend the first ANC visit to obtain IPTp1. Then the CHWs provided monthly doses of IPTp, submitted monthly reports, and continued to promote ANC. ANC attendance and IPTp uptake were monitored through monthly clinic and CHW reports. The catchment area populations were roughly the same, and monitoring showed that the additional provision of IPTp by CHWs resulted in more women being reached while at the same time ANC attendance remained high.
An endline su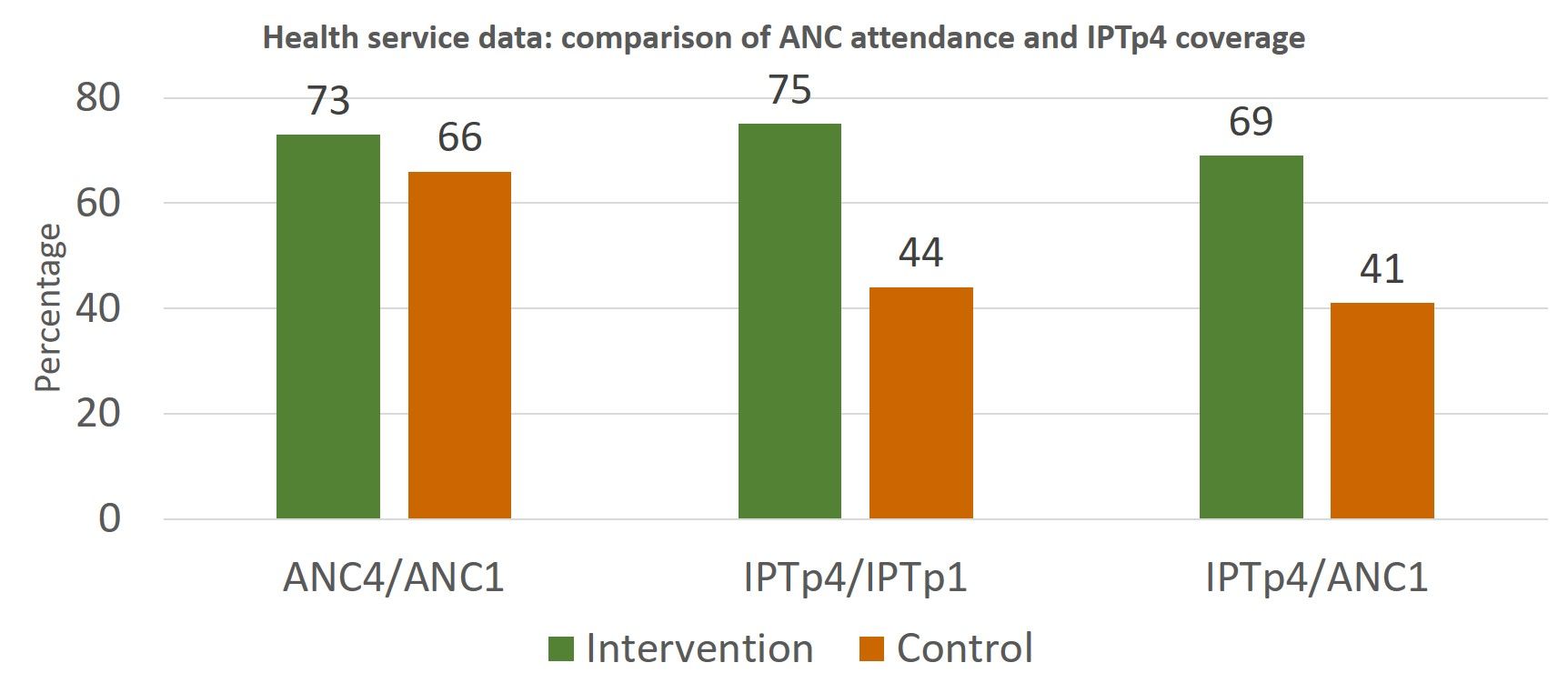 rvey was conducted after 18 months of implementation. Changes over time were compared between baseline and endline in intervention versus control villages. Attendance at ANC1 and ANC4 increased in both groups between baseline and endline but was significantly better for the intervention group. Likewise, coverage of IPTp3 and IPTp4 increased between baseline and endline for intervention and control women, but the difference was significant only in the intervention areas.
rvey was conducted after 18 months of implementation. Changes over time were compared between baseline and endline in intervention versus control villages. Attendance at ANC1 and ANC4 increased in both groups between baseline and endline but was significantly better for the intervention group. Likewise, coverage of IPTp3 and IPTp4 increased between baseline and endline for intervention and control women, but the difference was significant only in the intervention areas.
 Monthly monitoring of CHW and ANC registers and the household surveys both documented that community delivery of IPTp resulted in the desired increased uptake of services without detracting from ANC attendance. Community IPTp may be a promising strategy to improve coverage of IPTp.
Monthly monitoring of CHW and ANC registers and the household surveys both documented that community delivery of IPTp resulted in the desired increased uptake of services without detracting from ANC attendance. Community IPTp may be a promising strategy to improve coverage of IPTp.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Announcement &Case Management &CHW &Community &Ebola &Infection Prevention &IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 29 Oct 2018
Malaria Featured in Jhpiego Sessions at ASTMH 2018

Below is a list of Jhpiego Sessions at this week’s American Society of Tropical Medicine Annual Meeting in New Orleans (28 October-1 November). Please attend if you are at the conference:
![]() Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
- Poster Number 098: Performance of community health workers in providing integrated community case management services (iCCM) in 8 districts of Rwanda
- Poster 380: Contribution of quarterly malaria data review and validation to data quality and malaria services Improvement
- Poster LB-5117: Community based health workers can enhance coverage of intermittent preventive treatment of malaria in pregnancy and promote antenatal attendance
Poster Session B, Tuesday 30 October
- Poster 1088: Assessing organizational capacity to deliver quality malaria services in rural Liberia
- Poster 1092: Contribution of IMC project in transforming the face of malaria control for vulnerable populations in Burkina Faso
- Poster 1093: Malaria response plan in times of high transmission: An approach to improving the quality of hospital malaria management
- Poster 1111: Setting the stage to introduce a ground breaking approach to prevent malaria in pregnancy in Sub-Saharan Africa: baseline-readiness assessment findings from Democratic Republic of Congo, Mozambique, Madagascar, and Nigeria
- Poster 1337: Institutionalizing infection prevention and control practices in health facilities in Liberia following the Ebola epidemic
 Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Poster Session C, Wednesday 31 October
- Poster 1816: Experiences and perceptions of care seeking for febrile illness among caregivers and providers in 8 districts of Madagascar
- Poster 1818: Improving adherence to national malaria treatment guidelines by village health workers in selected townships through a low-dose, high-frequency training approach
- Poster 1819: Improving malaria case management through national roll-out of Malaria Service and Data Quality Improvement (MSDQI): A Case study from Tanzania
- Poster 1820: Collaborative quality improvement framework to support data quality improvement, experience from 10 collaborative facilities in Uganda
- Poster 1821: Using malaria death audits to improve malaria case management and prevent future malaria related preventable deaths
- Poster 1833: Multiple approaches for malaria case management in the struggle to reach pre-elimination of malaria.
Scientific Session 182, Thursday, November 1, 10:15 am – 12:00 p.m. Marriott – Balcony I,J,K – 3rd Floor: Seasonal malaria chemoprevention, an effective intervention for reducing malaria morbidity and mortality
CHW &Civil Society &Community &Health Systems &Partnership &Primary Health Care Bill Brieger | 28 Oct 2018
Achieving UHC through PHC Requires an Implementation Plan
 The new Astana Declaration says that, “We are convinced that strengthening primary health care (PHC) is the most inclusive, effective and efficient approach to enhance people’s physical and mental health, as well as social well-being, and that PHC is a cornerstone of a sustainable health system for universal health coverage (UHC) and health-related Sustainable Development Goals.” The Declaration outlined a vision, a mission, and a commitment. An opportunity to discuss how to implement this existed at the two-day conference in Astana Kazakhstan celebrating the 40th anniversary of the seminal Alma Ata Declaration.
The new Astana Declaration says that, “We are convinced that strengthening primary health care (PHC) is the most inclusive, effective and efficient approach to enhance people’s physical and mental health, as well as social well-being, and that PHC is a cornerstone of a sustainable health system for universal health coverage (UHC) and health-related Sustainable Development Goals.” The Declaration outlined a vision, a mission, and a commitment. An opportunity to discuss how to implement this existed at the two-day conference in Astana Kazakhstan celebrating the 40th anniversary of the seminal Alma Ata Declaration.
Ironically the opportunity was not fully grasped. There were many sessions that shared country experiences ranging from finance to information technology. Youth who will carry PHC forward for the next 40 years gave their opinions and thoughts. Lip-service as well as actual case examples of community involvement were featured. What we did not hear much of was the specifics of how countries, moving forward, will actually implement the commitments spelled out in the document.
 One colleague who has worked with the sponsoring agencies was of the view that since much advanced input and work from many partners and countries had gone into the new Declaration, which was already nicely printed, they were reluctant to provide the slightest chance that debate would be reopened.
One colleague who has worked with the sponsoring agencies was of the view that since much advanced input and work from many partners and countries had gone into the new Declaration, which was already nicely printed, they were reluctant to provide the slightest chance that debate would be reopened.
As they say, fair enough (maybe), but even if one takes the Declaration as a done deal, the matter if implementation needs to be addressed. There was ample criticism that the Alma Ata Declaration was not properly implemented. This was in part because academics and development agencies jumped the gun and pushed, with focused financial backing, what would be called selective primary health care that was more agency driven, not community directed as envisioned at Alma Ata (now Almaty) in 1978.
In order not to repeat those mistakes and give full voice to the community and key constituents, at minimum the implementation strategies of the pre-agreed Declaration should have been discussed in specific terms. Sure many ideas and examples were aired, but there was no attempt to focus these into workable strategies.
 But was the community even there in Astana to take part in strategizing? One community health worker from Liberia received much attention because she was the odd one out. Sure, there were plenty of NGOs, but not the real grassroots of civil society, although the youth involvement aspect of the conference approached that. Some of these NGOs and agencies had themselves been part of the selective PHC agenda.
But was the community even there in Astana to take part in strategizing? One community health worker from Liberia received much attention because she was the odd one out. Sure, there were plenty of NGOs, but not the real grassroots of civil society, although the youth involvement aspect of the conference approached that. Some of these NGOs and agencies had themselves been part of the selective PHC agenda.
There was plenty of talk about us involving them, especially when it came to community health workers (CHWs). CHWs should first be integrated into community systems to ensure they are accountable to communities. Then there should be an equal partnership between community systems and health systems. Otherwise CHWs get lost as just front line laborers.
Of course it is never too late. Regional gatherings may be a better forum that can discuss implementation in a more socially, economically and culturally appropriate way. Let’s hope we don’t look back in another 40 years and with the Astana Declaration had been better and more faithfully implemented.
Advocacy &Community &Leadership &Surveillance &Women Bill Brieger | 05 Jul 2018
Global Civil Society for Malaria Elimination (CS4ME)
 CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World
CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World  Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below.
Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below.
GLOBAL CIVIL SOCIETY FOR MALARIA ELIMINATION (CS4ME) DECLARATION
MALARIA WORLD CONGRESS 1ST-5TH JULY 2018
MELBOURNE, AUSTRALIA
Firm in the belief that empowered community and civil society are game-changers in health responses, we, representatives of national, regional and global malaria communities and civil society attending the First Malaria World Congress, have come together and formed the Global Civil Society for Malaria Elimination (CS4ME) as part of our commitment to joint advocacy for more effective, sustainable, people-centred, rights-based, equitable, and inclusive malaria programmes and Interventions.
At a time when the world has the resources and tools to prevent and treat malaria, it is unconscionable how people – mainly from impoverished, vulnerable and underserved communities – continue to die from the disease. While we commend the efforts of governments and the international community that brought the world closer to malaria elimination, we call for greater accountability, political will and action, resource investments, and sense of urgency to eliminate the disease.
CS4ME makes the following call to the governments of implementing countries, donor countries and other duty bearers:
FRAME MALARIA RESPONSES IN THE CONTEXT Of SOCIAL JUSTICE AND HUMAN RIGHTS, AND WITHIN UNIVERSAL HEALTH COVERAGE
Significant progress has been attained during the past 10 years to reduce the burden of malaria throughout the world and in working towards achieving malaria elimination. As countries enter into the elimination phase, we see again and again the epidemic concentrating among the most marginalised, remote, and disenfranchised communities. In South East Asia, the concentration of malaria among communities barred from accessing quality and affordable health services has accelerated the emergence of drug resistance that now threatens the wor1d at large. Everywhere, the last mile of elimination becomes a matter of access to health for impoverished and marginalised communities, in particular, refugees, ethnic minorities, indigenous communities, migrant and mobile populations – with many of the risks faced by these groups compounded further amongst women and girls.
Including the most local, represents a strategic investment contributing to appropriate, effective service delivery and people-driven surveillance and response.
We call on national governments, international institutions, bilateral and multilateral donors to prioritise and increase funding allocations for community-driven community and civil society initiatives. We request that specific funding streams be made available to community groups, and their access supported through peer-to-peer technical assistance.
Furthermore, we request that key performance indicators that enable accountability for bringing malaria services to the underserved be developed and implemented.
PARTNER WITH CIVIL SOCIETY AND COMMUNITY ACTORS FOR AN EFFECTIVE MALARIA SURVEILLANCE AND RESPONSE
As surveillance becomes an essential pillar for malaria elimination, the need for timely and robust data is increasingly critical. Essential evidence includes routine data, qualitative and quantitative research, as well as experience, lessons learned and the voices from affected communities. Support is required to build the ability of civil society to generate evidence, as well as to communicate it effectively to ensure that community-generated evidence will be able to influence decisions and result in sustained change.
To eliminate malaria, surveillance requires a response. Communities and civil society are the first responders, and will have the clearest insight Into what responses are effective in their context or on behalf of their constituents.
We demand that communities and civil society organisations be given equitable access to data and other information that can inform field-level response. We call for transparent information systems and multi-directional information flows in order to enable dialogue, and inform decisions at all levels. We urge the building up of surveillance systems that involve communities as analysts, advisors, decision-makers and responders.
We, malaria communities and civil society, offer our support, expertise, and lived experiences In contributing towards our shared vision of malaria elimination. We are fully committed to working alongside other stakeholders to build stronger, more inclusive and effective partnerships and sustainable responses towards elimination of malaria in this lifetime.
CHW &Community &ITNs &Ivermectin &Mapping &MDA &Seasonal Malaria Chemoprevention Bill Brieger | 04 Jul 2018
Mapping to Integrate Filariasis and Onchocerciasis Control with Malaria Interventions
William R Brieger (wbriege1@jhu.edu) and Gilbert Burnham (gburnha1@jhu.edu) of The Johns Hopkins Bloomberg School of Public Health, Department of International Health presented ideas about mapping and integration of neglected tropical diseases and malaria interventions at the Malaria World Congress, Melbourne, Australia, July 2018
Overview: Lymphatic Filariasis (LF) and Malaria share a common vector in sub-Saharan Africa. Mass Drug Administration (MDA) is a strategy that is common to both diseases. Where the diseases overlap there is the potential opportunity to coordinate both vector control and MDA to achieve synergy in program results. The example of Burkina Faso, supplemented with information from Ghana, serves as an example of what could be integrated and what actually happens.
 Background: Thirty years ago then veterinary drug, ivermectin, was found effective in controlling neglected tropical diseases (NTDs), specifically two human filarial diseases: onchocerciasis and lymphatic filariasis (LF). The drug manufacturer donates 300 million treatments annually to eliminate both diseases. Since then, annual community based mass drug administration (MDA) efforts have resulted in millions of treatments in endemic countries and great progress has been made toward elimination of transmission. Through observation and experimentation, ivermectin was found to kill malaria carrying mosquitoes when they bite people who have taken ivermectin making it a useful tool for vector control.
Background: Thirty years ago then veterinary drug, ivermectin, was found effective in controlling neglected tropical diseases (NTDs), specifically two human filarial diseases: onchocerciasis and lymphatic filariasis (LF). The drug manufacturer donates 300 million treatments annually to eliminate both diseases. Since then, annual community based mass drug administration (MDA) efforts have resulted in millions of treatments in endemic countries and great progress has been made toward elimination of transmission. Through observation and experimentation, ivermectin was found to kill malaria carrying mosquitoes when they bite people who have taken ivermectin making it a useful tool for vector control.

CHWs in Burkina Faso demonstrating how to measure height to determine ivermectin dosage
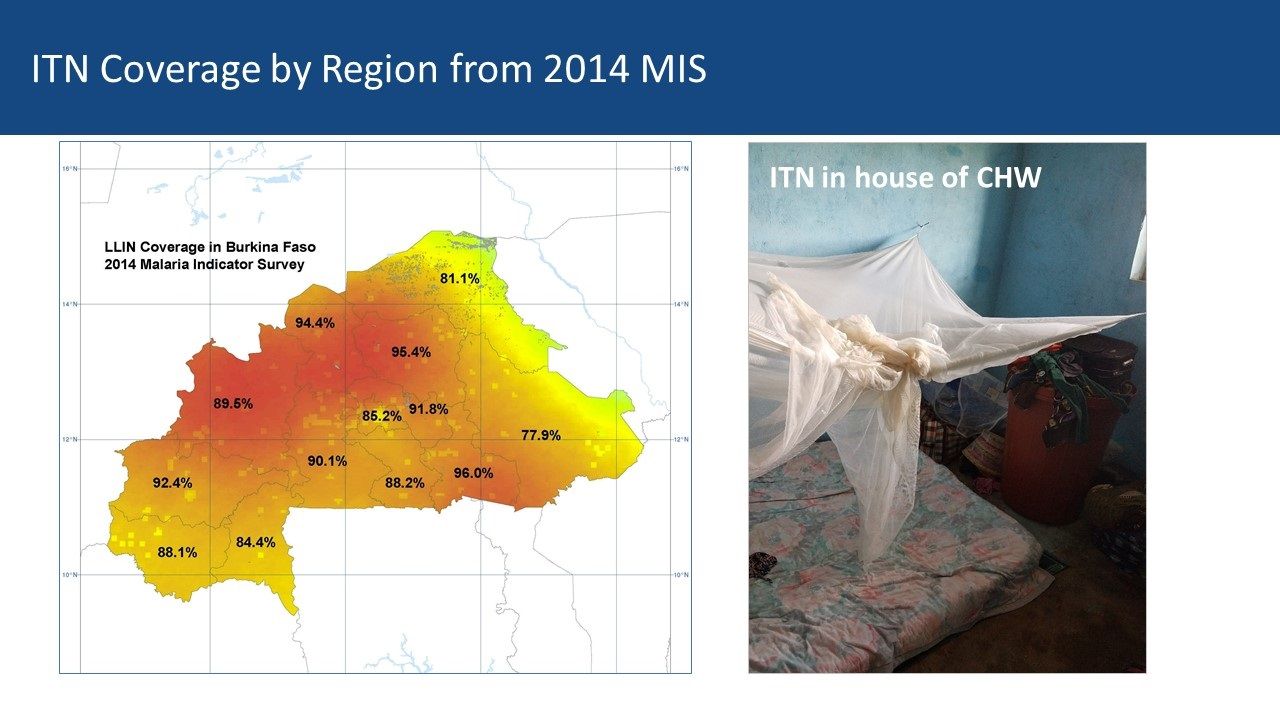
Community Health Workers’ Role: Current research is examining how dosing and timing of treatments may impact national malaria vector control efforts. Comparing maps between malaria and LF can be a starting point for adapting ivermectin MDAs for malaria vector control. Burkina Faso MDAs are operationalized by community health workers (CHWs) who are part of a national program that provides treatment for common illnesses and also conducts village level onchocerciasis and LF MDAs. Vector Control with Long Lasting Insecticide Treated Nets In most of rural Africa, malaria and lymphatic Filariasis are co-endemic and share the same anopheles mosquito vector.
However, that does not mean that there is a coordinated effort to plan distribution of LLINs despite the fact that the intervention meets the needs of both disease control efforts. The current NTD programs in Burkina Faso and Ghana focus on Preventive Chemotherapy (PCT) delivered through Mass Drug Administration (MDA). Vector Control is seen as essential in areas co-endemic with LF, Loa loa and Malaria – mapping helps identify priority areas for vector control.
 Vector Control by Chance: In Ghana, the NTD/LF elimination program was unaware of the LLIN coverage data available in the NMCP housed in an adjacent building. This illustrates the lack of collaboration between the two programs. Thus where — and if — vector control benefits the reduction of both diseases, it is often by chance where LF is concerned. The International NGO, The Carter Center, may be the only one that includes vector control as part of its programming for both malaria and LF in Nigeria. This practice should be replicated by other partners and country programs where possible.
Vector Control by Chance: In Ghana, the NTD/LF elimination program was unaware of the LLIN coverage data available in the NMCP housed in an adjacent building. This illustrates the lack of collaboration between the two programs. Thus where — and if — vector control benefits the reduction of both diseases, it is often by chance where LF is concerned. The International NGO, The Carter Center, may be the only one that includes vector control as part of its programming for both malaria and LF in Nigeria. This practice should be replicated by other partners and country programs where possible.
 Mass Drug Administration: MDA is the major strategy for control of five PCT diseases in the NTD program, and LF is one of those. Currently MDA anti-malarial drugs has been considered in limited situations in countries where there are areas that have very low transmission In the future countries may consider research that shows mosquitocidal effects of Onchocerciasis and LF MDAs with ivermectin. Otherwise for malaria, a special intervention called Seasonal Malaria Chemoprevention (SMC) is used in an MDA-like approach to reach young children in the African Sahel during high transmission months. In both cases, existing cadres of (usually volunteer) community health workers are the front line providers of MDA.
Mass Drug Administration: MDA is the major strategy for control of five PCT diseases in the NTD program, and LF is one of those. Currently MDA anti-malarial drugs has been considered in limited situations in countries where there are areas that have very low transmission In the future countries may consider research that shows mosquitocidal effects of Onchocerciasis and LF MDAs with ivermectin. Otherwise for malaria, a special intervention called Seasonal Malaria Chemoprevention (SMC) is used in an MDA-like approach to reach young children in the African Sahel during high transmission months. In both cases, existing cadres of (usually volunteer) community health workers are the front line providers of MDA.
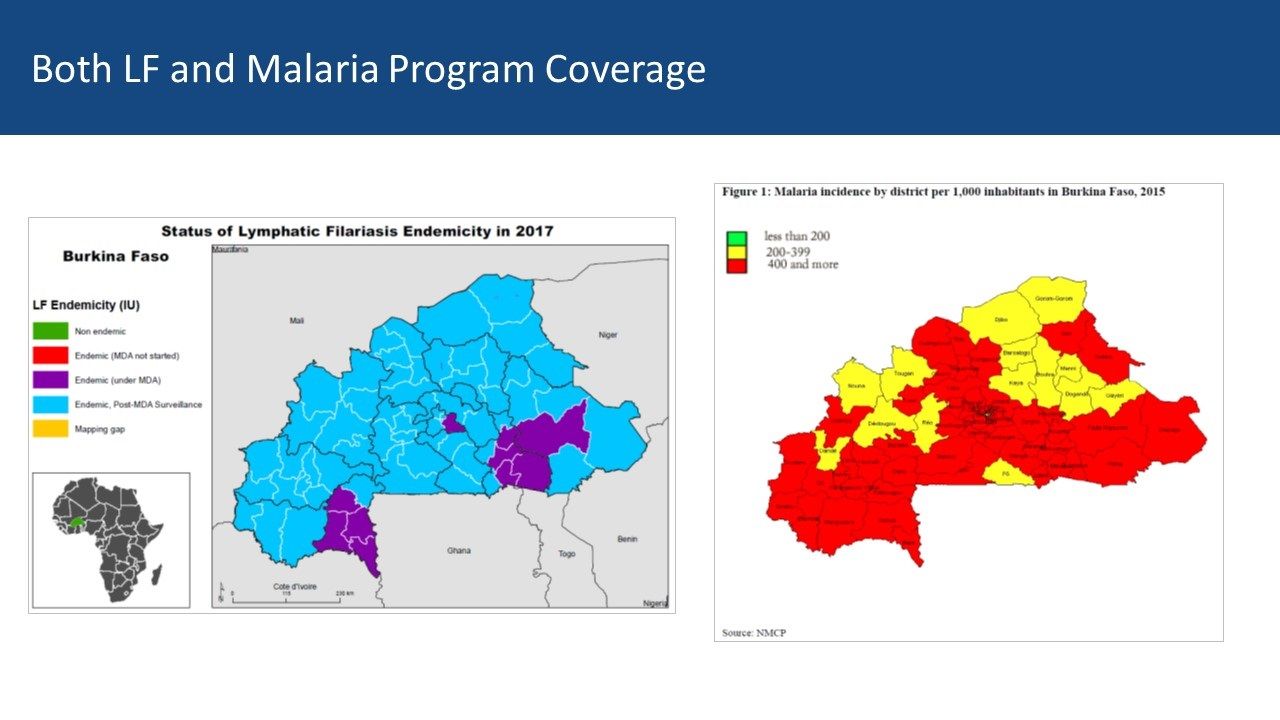
Burkina Faso LF Map from ESPEN: Mapping shows 10 of 70 health districts are currently doing LF MDA, though all have done it. Thus CHWs in all districts are experienced in ivermectin MDA. The malaria map shows that two-thirds of districts have a malaria incidence of 400/1000 or more while 14 have lower incidence. There is an overlap between current LF MDA districts and higher incidence malaria districts Both LF and Malaria Program Coverage can be seen to overlap in [program maps.

Ghana CHWs explain how they conduct MDA
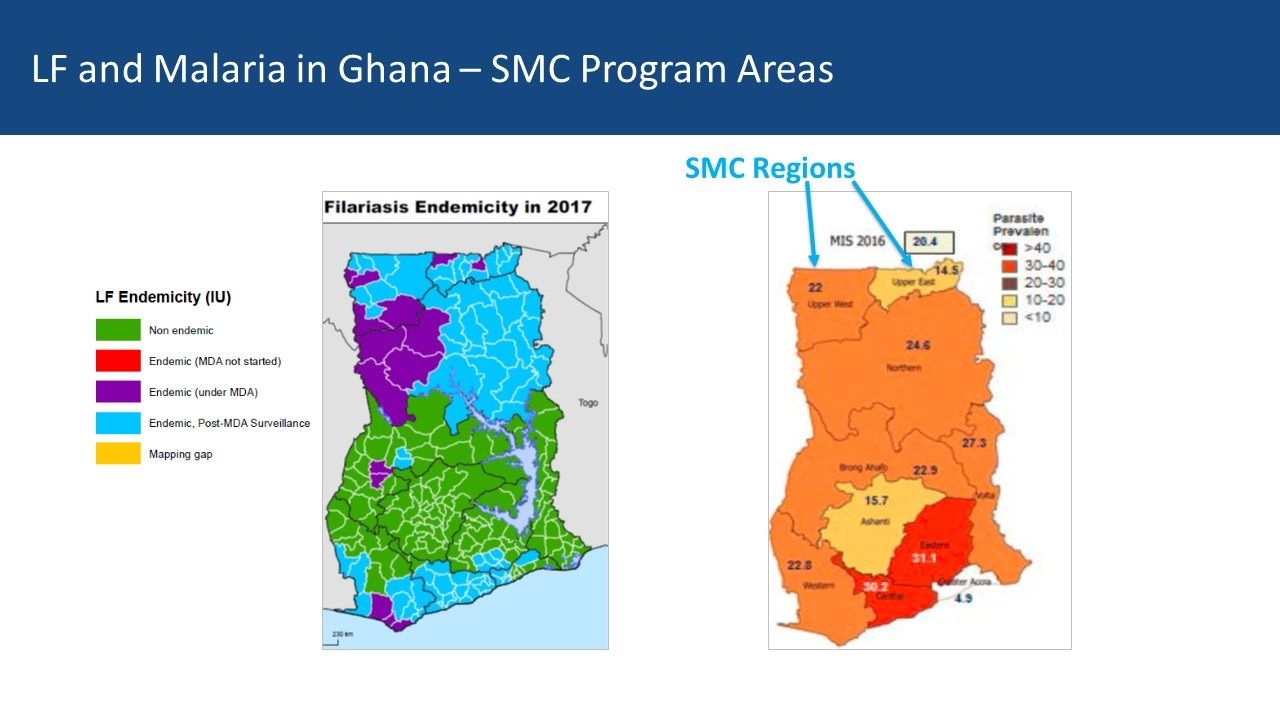
Ghana Experiences: Ghana provides a contrasting example. There five regions in central Ghana that are mostly non-endemic for LF but do have moderate malaria transmission In the south two regions with former LF MDA activity overlap with higher malaria endemicity While four northern regions have lower malaria parasite prevalence, they do have current and recent LF MDAs Community Directed Distributors work with LF MDA in Ghana
Conclusions: Malaria elimination will need a mix of strategies to be successful. Therefore, it is not too early for malaria and NTD program managers, as well as their respective donors, to begin comparing maps to identify possibilities for adapting ivermectin MDAs for malaria vector control. Even though one endemic disease is nearing control or elimination, the infrastructure put in place to accomplish this can be mobilized for other disease control efforts – as long as we map where interventions and resources have been targeted.
Advocacy &Case Management &Community &IPTp &ITNs Bill Brieger | 30 Apr 2018
Burkina Faso Celebrated World Malaria Day with Pledges to Defeat Malaria
 Burkina Faso celebrated World Malaria Day with pledges to Defeat Malaria on 25th April 2018. Dr Ousman Badolo. Technical Director of Jhpiego’s USAID/PMI Supported Improving Malaria Care (IMC) Project describes below the event in the village of Kamboinsin, not far from the capital, Ouagadougou. Ibrahim Sawadogo from IMC provided the photographs.
Burkina Faso celebrated World Malaria Day with pledges to Defeat Malaria on 25th April 2018. Dr Ousman Badolo. Technical Director of Jhpiego’s USAID/PMI Supported Improving Malaria Care (IMC) Project describes below the event in the village of Kamboinsin, not far from the capital, Ouagadougou. Ibrahim Sawadogo from IMC provided the photographs.
The day started with a proclamation of malaria day from Burkina Faso’s President, Roch Marc Christian Kaboré, to his assembled cabinet and the press. The president recognized that malaria is still a major public health issue in the country, and while deaths are decreasing, the incidence of malaria is not. The President called for a greater commitment of resources by all partners to insure that malaria can be defeated in Burkina Faso by 2030.
 Kamboinsin village in Sig-Noghin Health District was the site of further observances organized by the National Malaria Control Program, later that afternoon. This district was chosen because of having among the highest incidence rates for malaria in the region. Many partners set up booths to share their work in malaria with partners and citizens of the district. Included were three research centers (Centre Muraz, CNRFP and IRD), and three USAID programs supported by the President’s Malaria Initiative in Burkina Faso (Procurement and Supply Management [PSM], IMC and VectorLink), among others.
Kamboinsin village in Sig-Noghin Health District was the site of further observances organized by the National Malaria Control Program, later that afternoon. This district was chosen because of having among the highest incidence rates for malaria in the region. Many partners set up booths to share their work in malaria with partners and citizens of the district. Included were three research centers (Centre Muraz, CNRFP and IRD), and three USAID programs supported by the President’s Malaria Initiative in Burkina Faso (Procurement and Supply Management [PSM], IMC and VectorLink), among others.
 During the program both the Minister for Health and the US Ambassador spoke. The Minister highlighted the main strategies that Burkina Faso is employing to reduce and eliminate malaria including regular use of insecticide treated nets (ITN), seasonal malaria chemoprevention, Intermittent Preventive Treatment in Pregnancy (IPTp), Prompt and Appropriate Case Management and other Vector Control Strategies.
During the program both the Minister for Health and the US Ambassador spoke. The Minister highlighted the main strategies that Burkina Faso is employing to reduce and eliminate malaria including regular use of insecticide treated nets (ITN), seasonal malaria chemoprevention, Intermittent Preventive Treatment in Pregnancy (IPTp), Prompt and Appropriate Case Management and other Vector Control Strategies.
The US Ambassador shared a real-life story of a pregnant woman who during her current pregnancy decided to register early for Antenatal Care (ANC) as encouraged by the IMC project. She was able to get several doses of IPTp as required as well as obtain an ITN on her first visit, unlike in her previous pregnancies.
 Entertainment was provided by the comedian Hypolythe Wangrawa (alias M’ba Bouanga) who presented a sketch involving his ‘son’ who was not encouraging his wife to attend ANC and receive malaria prevention services. M’ba Bouanga chastised the son and an actor playing a midwife explained to the family the value of attending ANC and preventing malaria. Singers Maria Bissongo, Miss Oueora and Aicha Junior provided the audience with a song that embodied a variety of malaria prevention and care messages.
Entertainment was provided by the comedian Hypolythe Wangrawa (alias M’ba Bouanga) who presented a sketch involving his ‘son’ who was not encouraging his wife to attend ANC and receive malaria prevention services. M’ba Bouanga chastised the son and an actor playing a midwife explained to the family the value of attending ANC and preventing malaria. Singers Maria Bissongo, Miss Oueora and Aicha Junior provided the audience with a song that embodied a variety of malaria prevention and care messages.
 A highlight of the occasion was recognition of high performing health districts in the country. They were judged on criteria including good management of malaria commodity stocks, reduced case fatality rates, use of diagnostic tests to confirm malaria before treatment and coverage of at least three doses of IPTp. Four districts were given awards, Titao, Thyou, Boussouma and Batie, while Charles de Gaul Pediatric Hospital was also recognized.
A highlight of the occasion was recognition of high performing health districts in the country. They were judged on criteria including good management of malaria commodity stocks, reduced case fatality rates, use of diagnostic tests to confirm malaria before treatment and coverage of at least three doses of IPTp. Four districts were given awards, Titao, Thyou, Boussouma and Batie, while Charles de Gaul Pediatric Hospital was also recognized.
One can watch a video of the proclamation by the President on the National Facebook page. More details of the events are found in the following media: Lefaso.net and Paalga Observer.
World Malaria Day in Burkina Faso demonstrated the political will and commitment to “defeat malaria.” More and more national resources will be needed to reach the endline in 2030.
Advocacy &Case Management &Children &CHW &Community &Elimination &Funding &iCCM &Invest in Malaria Control &IPTp &ITNs Bill Brieger | 25 Apr 2018
On World Malaria Day the realities of resurgence should energize the call to ‘Beat Malaria’
 Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
 Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
 On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
 Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
 The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
In contrast a new form of IPT – seasonal malaria chemoprevention (SMC) for children in the Sahel countries has taken off with over 90% of children receiving at least one of the monthly doses during the high transmission season. Community case management is taking off as is increased use of rapid diagnostic testing. Increased access to care may explain how in spite of increased cases, deaths can be reduced. This situation could change rapidly if drug resistance spreads.
 While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
Twenty years after the formation of RBM and 70 years after the foundation of WHO, the children, families and communities of endemic countries are certainly ready to beat malaria. The question is whether the national and global partners are equally ready.
Community &Health Workers &Quality of Services Bill Brieger | 17 Apr 2018
Application d’un audit de la qualité des données (DQA) du paludisme dans le district sanitaire de Kribi, Cameroun
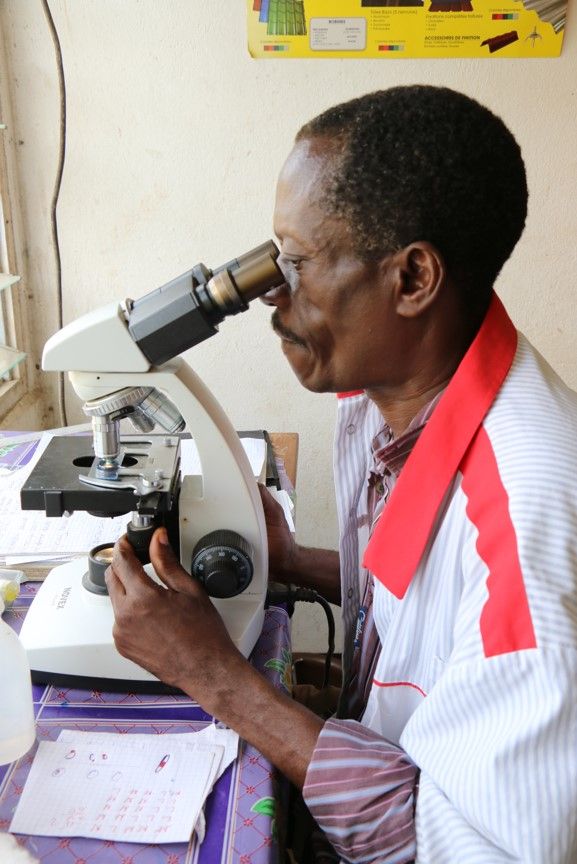 Kodjo Morgah, Naibei Mbaïbardoum, Mathurin Dodo, et Eric Tchinda from Jhpiego share their experiences in improving malaria data quality in Kribi District, Cameroon. The project was funded by the ExxonMobil Foundation. Their findings are presented below.
Kodjo Morgah, Naibei Mbaïbardoum, Mathurin Dodo, et Eric Tchinda from Jhpiego share their experiences in improving malaria data quality in Kribi District, Cameroon. The project was funded by the ExxonMobil Foundation. Their findings are presented below.
Les indicateurs clés du paludisme En 2015 dans le district sanitaire de Kribi, Cameroun, le mortalité palustre était 19% et le morbidité palustre était 29%. En outre, le couverture du premier traitement de TPI était 76% et 55% pour le deuxième.
 Les interventions du projet Amélioration de la qualité des services de contrôle du paludisme au Tchad et au Cameroun sont montrés dans le diagramme ci-joint.
Les interventions du projet Amélioration de la qualité des services de contrôle du paludisme au Tchad et au Cameroun sont montrés dans le diagramme ci-joint.
Les activités DQA ont commencé en 2012. Au début du projet, les formations sanitaires de Kribi ne disposaient pas d’une gestion des données suffisante en termes de fiabilité, de complétude et de promptitude des registres des formations sanitaires et des rapports soumis. En 2013 nous avons formé des prestataires de Kribi en prévention et traitement du paludisme, y compris la collecte et la gestion des données, et collaboration avec l’équipe cadre de district (ECD) du Ministère de la Santé Publique (MSP) pour institutionnaliser les réunions mensuelles de vérification et de validation des données. Puis en 2015 nous avons développé et diffusé d’affiches de suivi des données pour aider les formations sanitaires à suivre les indicateurs clés du paludisme afin de soutenir une prise de décision efficace. L’année passe, en 2017, le DQA est réalisé.
 Objectifs du DQA sont d’améliorer la qualité des données du paludisme dans le district de Kribi; identifier les erreurs systématiques; apprécier les sous-déclarations et/ou sur-déclarations; mesurer la concordance des données rapportées; apprécier la précision, la validité, la fiabilité, et la complétude des données collectées; et renforcer les capacités des ECD et du PNLP.
Objectifs du DQA sont d’améliorer la qualité des données du paludisme dans le district de Kribi; identifier les erreurs systématiques; apprécier les sous-déclarations et/ou sur-déclarations; mesurer la concordance des données rapportées; apprécier la précision, la validité, la fiabilité, et la complétude des données collectées; et renforcer les capacités des ECD et du PNLP.
Pour mettre en œuvre du DQA, nous avons sélectionné huit indicateurs du paludisme et un indicateur général. Le projet a adapté des outils de collecte des données développés par le projet MEASURE Evaluation financé par l’USAID. Puis, il a facilité le constitution et orientation des équipes d’évaluateurs des données composées du personnel de Jhpiego et des membres de l’ECD. Apres ça, les équipes commencent le réalisation du DQA dans des sites sélectionnés
Modalités :
- Aucun problème de qualité des données, si la mDA est comprise entre 100% et 90%
- Problèmes mineurs de qualité des données, si la mDA est comprise entre 89% et 70%
- Problèmes majeurs de qualité des données, si la mDA est inférieure à 70%
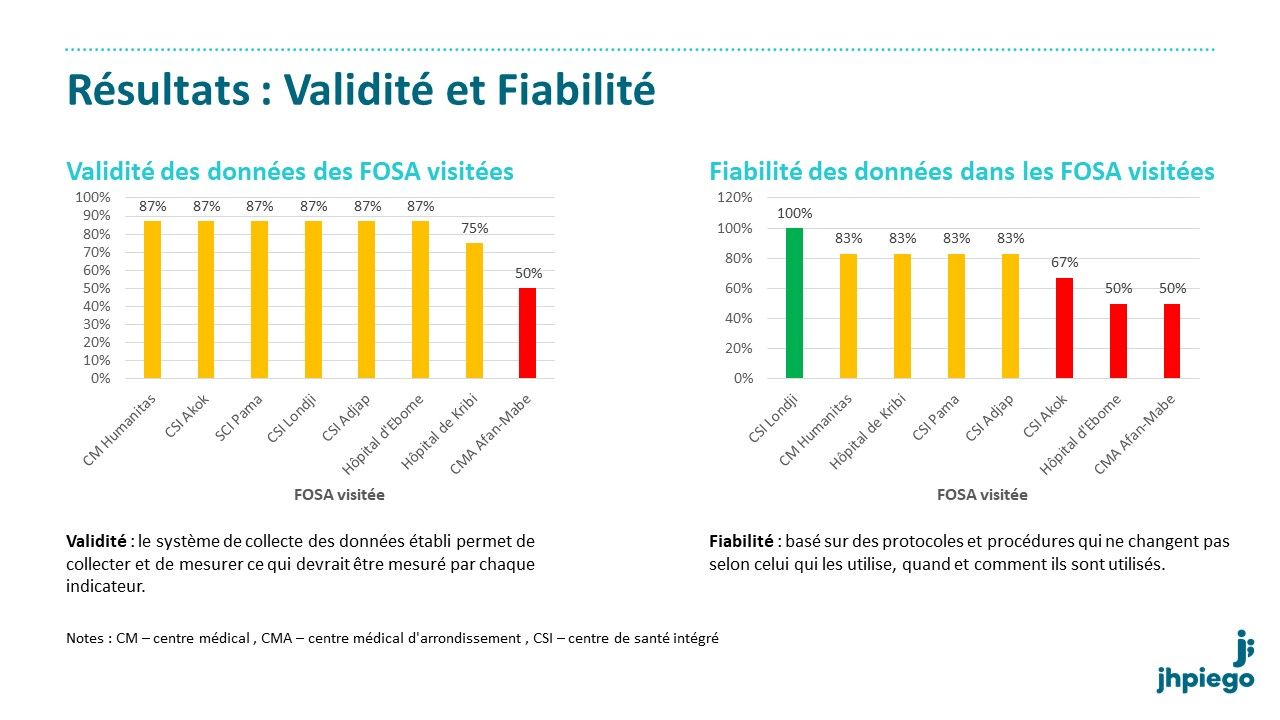
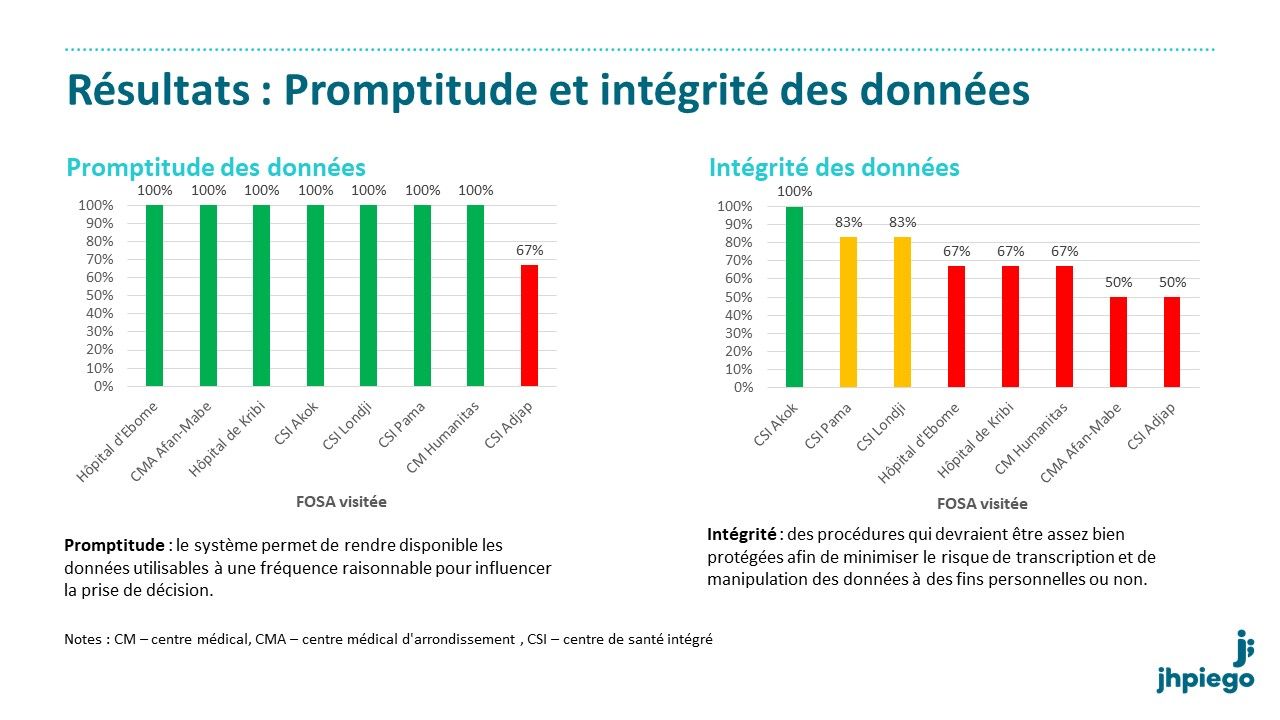


Conclusions: Le DQA a réussi à identifier les problèmes qui ont affecté la qualité des données dans les formations sanitaires de Kribi. Il a aussi révélé une meilleure qualité des données dans les formations sanitaires rurales que dans les formations sanitaires urbaines. Dans l’ensemble, la qualité des données du paludisme est acceptable dans la majorité des formations sanitaires soutenues par le projet.
 L’équipe de projet doit soutenir le personnel et les formations sanitaires du MS du district dans l’intégration des recommandations du DQA pour continuer à améliorer la qualité des données.
L’équipe de projet doit soutenir le personnel et les formations sanitaires du MS du district dans l’intégration des recommandations du DQA pour continuer à améliorer la qualité des données.
Recommendations: Il est necessaire de renforcer les capacités des prestataires dans la collecte des données à travers la supervision formative. Dans l’outil de supervision de district, il est utile d’intégrer la vérification et le contrôle des données. Une Aide-mémoire sur la vérification, le contrôle et la validation des données du paludisme devrait être disponible.
Community &Primary Health Care Bill Brieger | 13 Apr 2018
Malaria and Primary Health Care: 40 Years after Alma Ata
The Concept of Primary Health Care (PHC) was formalized in 1978 when The World Health Organization and UNICEF convened a major conference in the then Alma Ata in Kazakhstan. The resulting Alma Ata Declaration resulted in advocacy for Health for All, which had evolved into Universal Health Coverage. The Declaration outlined important principles such as community participation in health care planning and delivery, promotion of scientifically sound and acceptable health interventions, the use of community-based health workers (CHWs), and addressing the common endemic health problems in each community. One of those endemic problems common to a majority of communities in Africa is malaria. Now in 2018, 40 years after the Alma Ata Declaration we explore how malaria has progressed within the context of PHC.
 The Roll Back Malaria Partnership (RBM) began in 1998, 20 years after Alma Ata. When RBM convened a meeting of African Heads of State in 2000 the resulting Abuja Declaration set targets for major malaria interventions of 80% coverage by 2010. The Abuja Declaration reflected principles of Alma Ata when it called on all member states to undertake health systems reforms which will:
The Roll Back Malaria Partnership (RBM) began in 1998, 20 years after Alma Ata. When RBM convened a meeting of African Heads of State in 2000 the resulting Abuja Declaration set targets for major malaria interventions of 80% coverage by 2010. The Abuja Declaration reflected principles of Alma Ata when it called on all member states to undertake health systems reforms which will:
- Promote community participation in joint ownership and control of Roll Back Malaria actions to enhance their sustainability.
- Make diagnosis and treatment of malaria available as far peripherally as possible including home treatment.
- Make appropriate treatment available and accessible to the poorest groups in the community.
By 2011 reality intervened. WHO reported that “In the 10 years that has passed since the Abuja Declaration, there has been progress towards increasing the availability of financial resources for health at least in terms of dollar values. However, there has not been appreciable progress in terms of the commitments the Africa Union governments make to health, or in terms of the proportion of GNI the rich countries devote to Overseas Development Assistance.” Since that time funding from international and bilateral donors has leveled, such that there is even greater need for malaria endemic countries to step forward and guarantee access to malaria prevention and treatment services are available through PHC at the grassroots. Such access needs to move beyond removing barriers to making malaria interventions attractive to the community.

Community Health Workers in Nigeria are trained to provide malaria community case management
Christopher and colleagues looked to the community and examined how response to malaria and other childhood illnesses were faring 30 years since Alma Ata. After they reviewed seven studies of community health workers they concluded that “CHWs in national programmes achieved large mortality reductions of 63% and 36% respectively, when insecticide-treated nets and anti-malarial chemoprophylaxis were delivered, in addition to curative interventions.” (They found little evidence of the effectiveness of these community interventions on pneumonia and diarrhoea.) The challenge they saw was the ability of countries to move beyond successful studies to scale up and sustain community malaria control interventions to the national level and thereby reap the full promises and benefits of PHC.
Others continue to advocate for a community role in achieving malaria goals through PHC. Malaria Consortium has looked at the position of malaria control within the context of Community Based PHC (CBPHC) and the use of CHWs as a means for revisiting Health for All.

Community donates a house in Western Region Ghana to serve as CHPS Compound where malaria services are provided to the community
Ghana’s community-based health planning and services (CHPS) program aims to make primary care accessible at the grass roots. CHPS compounds are small clinics in space usually donated by the community, staffed by community health officers who oversee community based agents (CBAs) and other community volunteers who treat and prevent malaria through integrated community case management. Countries have also build on the community directed intervention approach pioneered by the African Program for Onchocerciasis Control to ensure malaria interventions are delivered through community community planning and action.
Controlling and eventually eliminating malaria will certainly go a long way toward helping achieve Health for All. On this 40th Anniversary year of Alma Ata it is time to ensure that all malaria endemic countries and malaria donors revisit the basic philosophy of community action and participation and ensure that these principals guide us to accessible and sustainable malaria programming by the community “Through their Full Participation.”
![]() (This posting has been extracted from a full article appearing in the April 2018 Issue of Africa Health. Also please join the discussion about Alma Ata at 40 on the forum created by colleagues at the Johns Hopkins Bloomberg School of Public Health.)
(This posting has been extracted from a full article appearing in the April 2018 Issue of Africa Health. Also please join the discussion about Alma Ata at 40 on the forum created by colleagues at the Johns Hopkins Bloomberg School of Public Health.)
CHW &Community &Equity &Health Workers &ITNs Bill Brieger | 12 Mar 2018
Malaria by the numbers: are the statistics real or are they a barrier to community involvement?
 George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
——-
 I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
Today malaria is still among the top causes of infant mortality in many African countries, including Ghana, yet we have mosquito nets, coils, sprays, long sleeved shirts that have been circulating in the country for years……and sometimes I wonder: why?
Total funding for malaria prevention and control was 2.7 billion dollars in 2016. Between 2014-2016, 582 million nets were distributed, of which 505 million were distributed in Africa, yet the number of malaria cases increased from 211 million in 2015 to 216 million in 2016 (WHO-malaria fact sheet, 2017).
I was once a supervisor for the distribution of long-lasting insecticide treated nets in rural communities. The numbers driven world saw big numbers that showed that many pregnant women were not sleeping under mosquito nets and so the solution to solve the malaria problem was to give them mosquito nets.
 First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
This time we went into a house with a hammer, nails and ropes, and families showed us their bedroom and we hung the net for them. And yet malaria still rules. What happened with the free bed nets is now widely reported across different countries in Africa.
What do the numbers we measure mean to the people they represent?
 As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
Frustrations abound on both ends of the system, for public health agents and community members. Numbers act as the barrier between the two ends of the “system”, and our goal must be to break the barrier. The numbers that drive interventions can be meaningless to the community people they represent unless we engage the community and learn how our interventions can really help them.