Case Management &CHW &IPTp &ITNs Bill Brieger | 14 Apr 2018
Community Health Volunteers Contribute to Improved Malaria Prevention and Management in Kribi, Cameroon
Kodjo Morgah, Eric Tchinda, and Naibei Mbaïbardoum of Jhpiego (a Johns Hopkins University Affiliate) in Cameroon are presenting a poster at the Multilateral Initiative for Malaria Conference in Dakar this week. Their findings, seen below, show how community health volunteers can contribute to improving the quality of malaria control services in Chad and Cameroon.

CHV Lilian Kubeh preparing to administer a rapid diagnostic test. Photo by Karen Kasmauski.
Project objectives focused overall on contributing to the reduction of malaria-related morbidity and mortality in Cameroon and Chad. It also aimed to strengthen community-based interventions through the use of community health volunteers (CHVs) to manage simple cases of malaria and conduct awareness-raising activities. The geographic scope of the project was Kribi District in the south of Cameroon. Thirty-two health facilities are supported by Jhpiego. Kribi District has an estimated population of 134,876.
Reports from the National Malaria Control Program show that malaria is the leading cause of morbidity in Cameroon—an estimated 1,500,000 cases occur each year. In 2016, it was the leading reason for medical consultations (23.6% of all medical consultations) and hospitalizations (46% of all hospitalizations). Among children under 5 years of age, malaria accounted for 41% of all medical consultations and 55% of all hospitalizations. Malaria is also a leading cause of mortality. In 2016, Cameroon had 2,639 deaths caused by malaria—12% of all deaths across all age groups and 28% of all deaths among children under 5 years of age were attributed to malaria.
 Project intervention strategies target the four levels of the health system. The CHV intervention was mobilized to support the strategy at the community level as seen in the attached diagram. In 2012 and 2014, 38 CHVs were selected by the community and received training to support areas in the district more than 10 km from a health center. (Note: 10 km was the measurement tool used to determine the geographic scope of each CHV for this project.) An initial donation of medications, data collection tools, and small equipment was made available to CHVs using funding from ExxonMobil Foundation. An evaluation of the training intervention was conducted by an external consultant in April 2016.
Project intervention strategies target the four levels of the health system. The CHV intervention was mobilized to support the strategy at the community level as seen in the attached diagram. In 2012 and 2014, 38 CHVs were selected by the community and received training to support areas in the district more than 10 km from a health center. (Note: 10 km was the measurement tool used to determine the geographic scope of each CHV for this project.) An initial donation of medications, data collection tools, and small equipment was made available to CHVs using funding from ExxonMobil Foundation. An evaluation of the training intervention was conducted by an external consultant in April 2016.

CHV Daniel Ze conducting an individual educational session on IPTp. Photo by Karen Kasmauski.
CHVs conduct outreach activities in their communities—via home visits and community education sessions—to provide health education on malaria transmission and prevention, use of long-lasting insecticidal nets, the importance of intermittent preventive treatment in pregnancy (IPTp), and the importance of promptly seeking medical care for suspected cases of malaria. CHVs also support national health campaigns and health promotion events, including World Malaria Day. In Cameroon, where CHVs are also able to test and treat patients, they administer rapid diagnostic tests (RDTs) and treat cases of uncomplicated malaria.
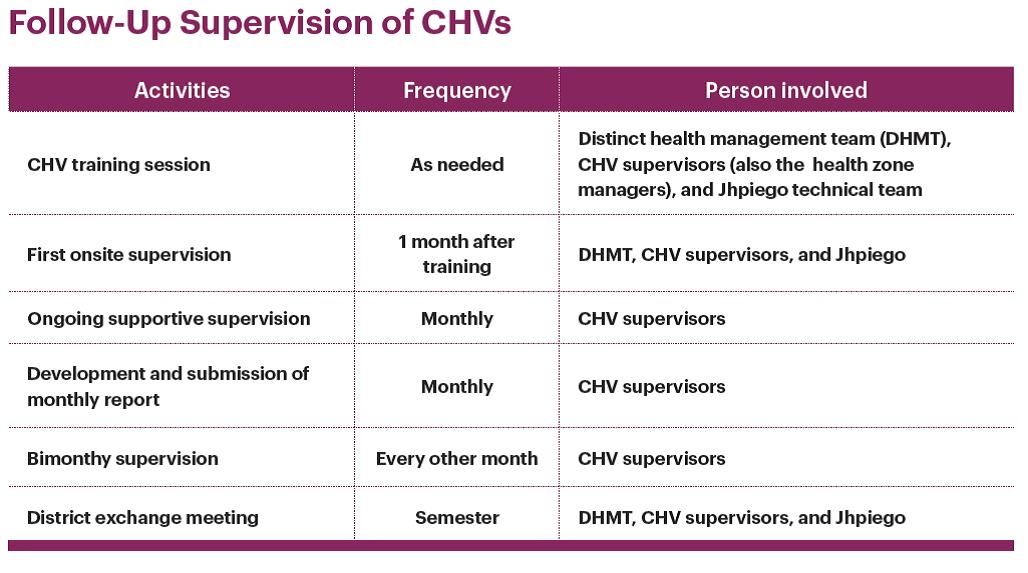 Motivation of CHVs included ongoing training and technical updates, regular replenishment of materials, CHVs are recognized and respected community leaders, provision of per diem and transport costs, and continued advocacy targeting district officials to provide CHV stipends to ensure sustainability. Attached are details of the supervisory activities that provided continual technical support to the CHVs to ensure that they retain knowledge and skills to carry out their activities and track their data.
Motivation of CHVs included ongoing training and technical updates, regular replenishment of materials, CHVs are recognized and respected community leaders, provision of per diem and transport costs, and continued advocacy targeting district officials to provide CHV stipends to ensure sustainability. Attached are details of the supervisory activities that provided continual technical support to the CHVs to ensure that they retain knowledge and skills to carry out their activities and track their data.
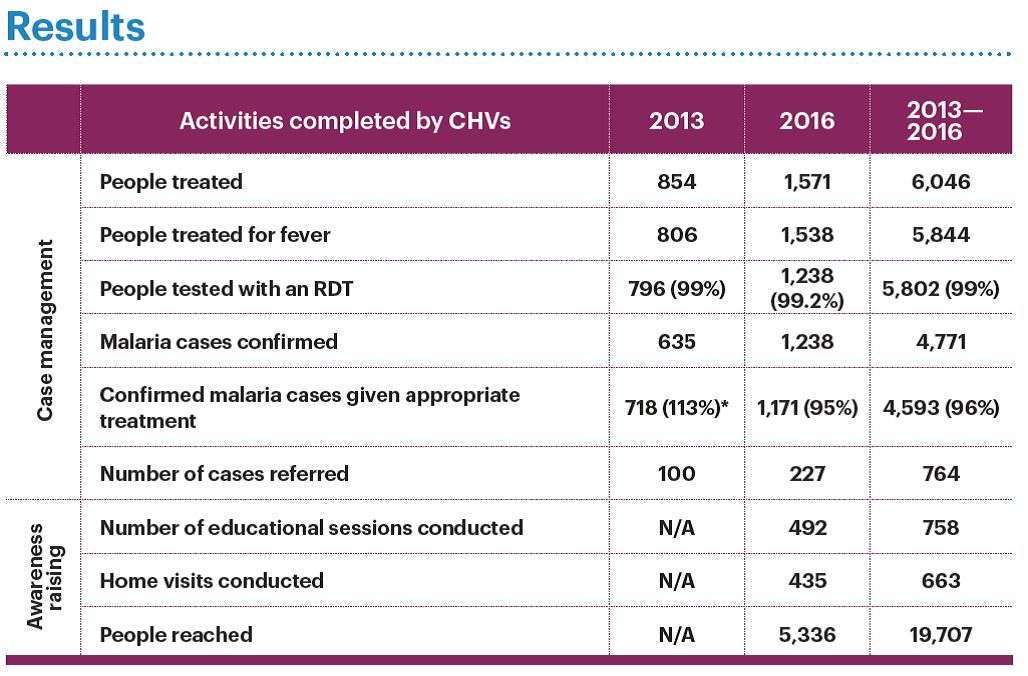 Between 2013 and 2016 CHVs in these communities were able to reach nearly 20,000 people with a variety of malaria services as seen in the attached table. The project paid close attention to data quality, which was reviewed with the CHVs on a regular basis, resulting in improved data quality. CHVs improved the accessibility of malaria prevention and care services for communities living in remote areas. Results from April 2016 external evaluation show these results. Knowledge of malaria prevention is significantly higher in households that did not receive CHV support (p = 0.001). Use of long-lasting insecticide-treated nets is higher in households that benefitted from CHV support (88%) than in households that did not benefit from CHV support (73%) (p = 0.023). There was an increase in the delivery of IPTp2, from 60% in 2012 to 70% in 2016.
Between 2013 and 2016 CHVs in these communities were able to reach nearly 20,000 people with a variety of malaria services as seen in the attached table. The project paid close attention to data quality, which was reviewed with the CHVs on a regular basis, resulting in improved data quality. CHVs improved the accessibility of malaria prevention and care services for communities living in remote areas. Results from April 2016 external evaluation show these results. Knowledge of malaria prevention is significantly higher in households that did not receive CHV support (p = 0.001). Use of long-lasting insecticide-treated nets is higher in households that benefitted from CHV support (88%) than in households that did not benefit from CHV support (73%) (p = 0.023). There was an increase in the delivery of IPTp2, from 60% in 2012 to 70% in 2016.
In conclusion CHVs have increased their communities’ access to health centers through referrals, health education on malaria prevention, IPTp, and treatment for simple and severe cases of malaria. Regular supervision of CHVs by their supervisors (the health zone managers) is essential to maintaining and strengthening CHV performance and motivation. Continuing advocacy efforts with local authorities is necessary to ensure that CHV activities are sustainable. The project team aims to establish a mechanism to improve documentation of its activities to better measure the impact on indicators at the community, facility, and district levels, and provide evidence for advocacy to sustain these efforts.
Case Management &CHW &Elimination &Malaria in Pregnancy Bill Brieger | 11 Apr 2018
Multilateral Initiative for Malaria (MIM) – Jhpiego Presents in Dakar
 The 7th Pan African Malaria Conference holds from 15-20 April 2017, Dakar, Senegal. The conference celebrates 20 years since the initial establishment of the Multilateral Initiative on Malaria (MIM) by the Tropical Disease Research Program and partners.
The 7th Pan African Malaria Conference holds from 15-20 April 2017, Dakar, Senegal. The conference celebrates 20 years since the initial establishment of the Multilateral Initiative on Malaria (MIM) by the Tropical Disease Research Program and partners.
During the conference next week, staff from Jhpiego malaria projects in Burkina Faso, Liberia, Nepal, Madagascar and Cameroon will share oral and poster presentations to highlight their work. Below is a list along with the location numbers.
- Application d’un Audit de la Qualité des données (DQA) du paludisme dans le District Sanitaire de Kribi, Cameroun, SS-13 Oral
- Contribution des Agent de Santé Communautaire (ASC) à l’amélioration de la prévention et la prise en charge du paludisme dans le district de Kribi, Cameroun, B-40 Poster
- MOH’s effort in developing and implementing Quality Assurance plan (QAP) for Global Fund-supported antimalarial drugs: A case study of Nepal in the context of malaria elimination, C-107 Poster
- Community-Based Health Workers in Burkina Faso: Are they ready to take on a larger role to prevent malaria in pregnancy? D-115 Poster

- Contribution of Community-Based Health Workers (CBHWs) to Improving Prevention of Malaria in Pregnancy in Burkina Faso: Review of health worker perceptions from the baseline study D-118 Poster
- Malaria in Pregnancy: The Experience of MCSP in Liberia, D-140 Poster
- Improved Malaria Case Management of Under-Five Children: The Experience of MCSP-Restoration of Health Liberia project D-141 Poster
- Experiences and perceptions of care seeking for febrile illness among caregivers, pregnant women and health providers in eight districts of Madagascar D-142 Poster

 Abstracts will be shared here on the day of each presentation for those unable to attend MIM. Also check Jhpiego at Exhibit Booth 148.
Abstracts will be shared here on the day of each presentation for those unable to attend MIM. Also check Jhpiego at Exhibit Booth 148.
CHW &Diagnosis &Elimination &Epidemiology Bill Brieger | 01 Apr 2018
Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia
Global Health Day 2018 sponsored by the Johns Hopkins University Center for Global Health featured a poster presentation by several colleagues on Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia. Fiona Bhondoekhan, William Moss, Timothy Shields, Douglas Norris, Kelly Searle, Jennifer Stevenson, Harry Hamapumba, Mukuma Lubinda and Japhet Matoba (Southern Africa International Centers of Excellence in Malaria Research, the JHU Bloomberg School of Public Health, and the Macha Research Trust, Zambia) share their findings below.
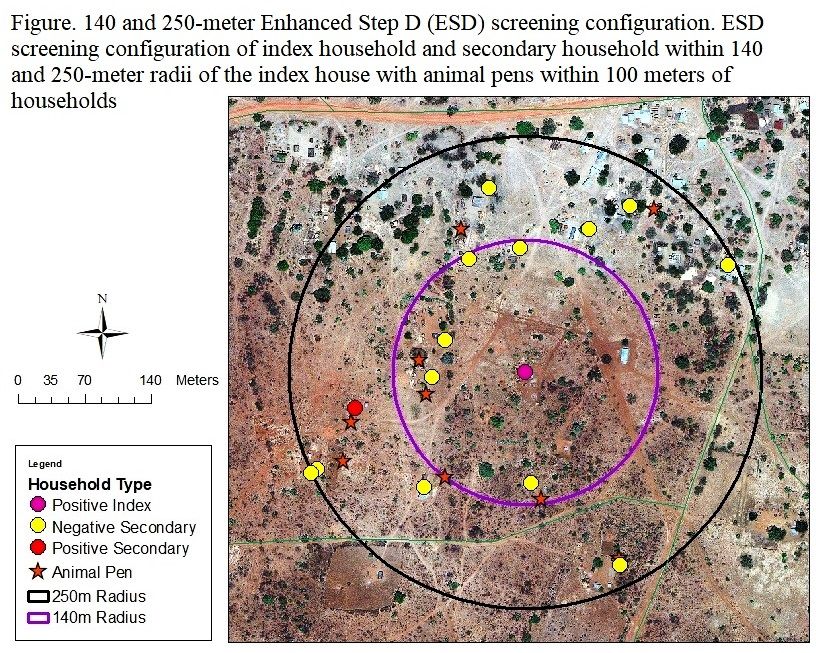 Background: Malaria screen-and-treat (called Step D in Zambia) is a reactive case detection strategy in which cases detected at a health center trigger community health workers (CHWs) to screen for secondary malaria cases within a 140-meter radius of the index case household using PfHRP2 rapid diagnostic tests (RDTs). Few studies evaluated whether an evidence-based strategy using environmental features that characterize the immediate surroundings of a household, can improve the efficiency of secondary case identification.
Background: Malaria screen-and-treat (called Step D in Zambia) is a reactive case detection strategy in which cases detected at a health center trigger community health workers (CHWs) to screen for secondary malaria cases within a 140-meter radius of the index case household using PfHRP2 rapid diagnostic tests (RDTs). Few studies evaluated whether an evidence-based strategy using environmental features that characterize the immediate surroundings of a household, can improve the efficiency of secondary case identification.
Objective: This study utilized the Step D and extended the screening radius to 250-meters (termed Enhanced Step D or ESD) to assess which local environmental variables can guide CHWs to identify secondary cases more efficiently. As Zambia works toward eliminating malaria, more refined and targeted case detection strategies are required to find the untreated malaria cases that could serve as potentially asymptomatic sources of infection. This study can help guide and plan reactive case detection strategies in Zambia that allow community health workers/field teams to employ an evidence-based strategy to find malaria-positive secondary households situated near index case houses more efficiently.
 Methods: Demographic information, malaria diagnosis, bed-net use and ownership, cooking energy source, and household floor material were obtained from surveys. Households were stratified into malaria positive and negative secondary households using RDT and qPCR results. ArcGIS was used to generate the following local environmental variables: screening radius (140 vs. 250-meters), number of animal pens within 100-meters, distance to nearest animal pen, distance and elevation difference between index and secondary houses, as well as the following large scale environmental variables: distance to main road and nearest stream category. Generalized estimating equations (GEE) estimated the cross-sectional effect for the difference in odds of a positive vs. negative secondary household for each predictor. For the secondary analysis GEE with the same model specifications was used to estimate the cross-sectional difference in odds of a positive vs. negative household for each environmental predictor. Model fit was evaluated with the Hosmer-Lemeshow goodness of fit test and significance was evaluated as a p-value of 0.05. Statistical analyses were carried out using STATA 14.2.
Methods: Demographic information, malaria diagnosis, bed-net use and ownership, cooking energy source, and household floor material were obtained from surveys. Households were stratified into malaria positive and negative secondary households using RDT and qPCR results. ArcGIS was used to generate the following local environmental variables: screening radius (140 vs. 250-meters), number of animal pens within 100-meters, distance to nearest animal pen, distance and elevation difference between index and secondary houses, as well as the following large scale environmental variables: distance to main road and nearest stream category. Generalized estimating equations (GEE) estimated the cross-sectional effect for the difference in odds of a positive vs. negative secondary household for each predictor. For the secondary analysis GEE with the same model specifications was used to estimate the cross-sectional difference in odds of a positive vs. negative household for each environmental predictor. Model fit was evaluated with the Hosmer-Lemeshow goodness of fit test and significance was evaluated as a p-value of 0.05. Statistical analyses were carried out using STATA 14.2.
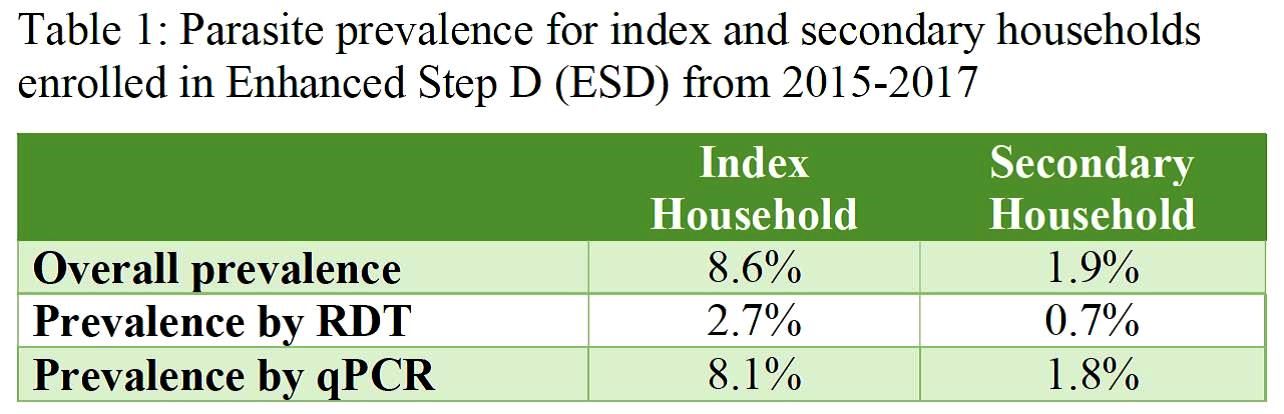
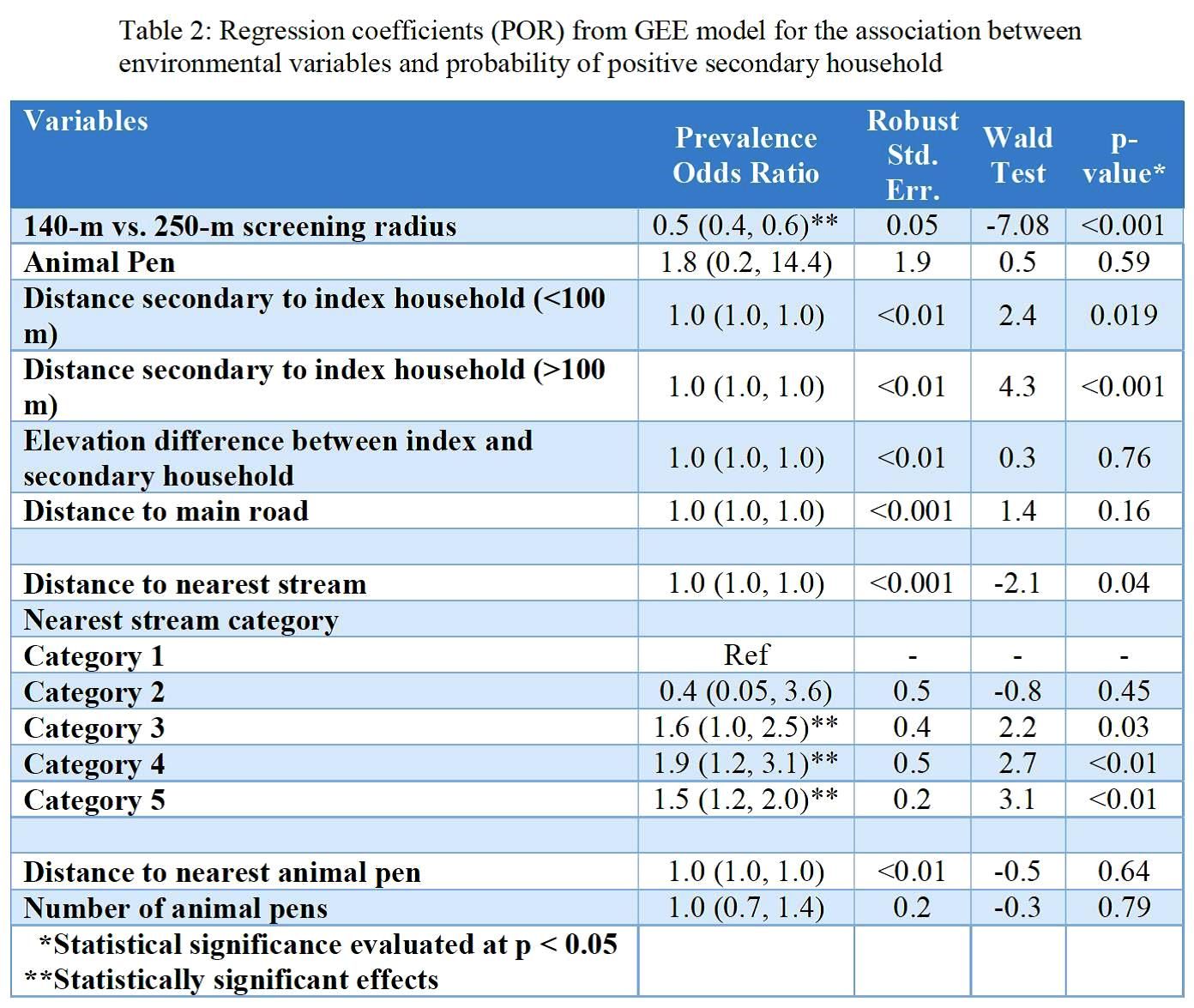 Results: Screening within the index households yielded an overall parasite prevalence of 8.6%, which was higher by qPCR (8.1%) than RDT (2.7%) as seen in Table 1. Secondary households had an overall parasite prevalence of 1.9% with similar differences by test used. Key results from regression analysis seen in Table 2 include a difference in prevalence according to screening radius as well as by proximity to the nearest stream. Secondary analysis produced similar results but showed statistically significant higher odds for households where animal pens were present.
Results: Screening within the index households yielded an overall parasite prevalence of 8.6%, which was higher by qPCR (8.1%) than RDT (2.7%) as seen in Table 1. Secondary households had an overall parasite prevalence of 1.9% with similar differences by test used. Key results from regression analysis seen in Table 2 include a difference in prevalence according to screening radius as well as by proximity to the nearest stream. Secondary analysis produced similar results but showed statistically significant higher odds for households where animal pens were present.
Conclusion: Screening for secondary households within low-transmission setting in Zambia could be optimized by using both local-scale indicators such as the presence of animal pens and large-scale indicators such as streams as environmental guiding tools.
Acknowledgements: This research was supported in part the Bloomberg Philanthropies and the Johns Hopkins Malaria Research Institute, and the NIH-sponsored Southern and Central Africa ICEMR 2U19AI089680.

CHW &Community &Equity &Health Workers &ITNs Bill Brieger | 12 Mar 2018
Malaria by the numbers: are the statistics real or are they a barrier to community involvement?
 George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
——-
 I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
Today malaria is still among the top causes of infant mortality in many African countries, including Ghana, yet we have mosquito nets, coils, sprays, long sleeved shirts that have been circulating in the country for years……and sometimes I wonder: why?
Total funding for malaria prevention and control was 2.7 billion dollars in 2016. Between 2014-2016, 582 million nets were distributed, of which 505 million were distributed in Africa, yet the number of malaria cases increased from 211 million in 2015 to 216 million in 2016 (WHO-malaria fact sheet, 2017).
I was once a supervisor for the distribution of long-lasting insecticide treated nets in rural communities. The numbers driven world saw big numbers that showed that many pregnant women were not sleeping under mosquito nets and so the solution to solve the malaria problem was to give them mosquito nets.
 First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
This time we went into a house with a hammer, nails and ropes, and families showed us their bedroom and we hung the net for them. And yet malaria still rules. What happened with the free bed nets is now widely reported across different countries in Africa.
What do the numbers we measure mean to the people they represent?
 As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
Frustrations abound on both ends of the system, for public health agents and community members. Numbers act as the barrier between the two ends of the “system”, and our goal must be to break the barrier. The numbers that drive interventions can be meaningless to the community people they represent unless we engage the community and learn how our interventions can really help them.
CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 07 Nov 2017
Potential Contribution of Community-Based Health Workers to Improving Prevention of Malaria in Pregnancy
 Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Danielle Burke, and Bill Brieger of Jhpiego have designed and are implementing a study to determine the effect of delivering Intermittent Preventive Treatment for Malaria in Pregnancy through community health workers in Burkina Faso with the support of the US President’s Malaria Initiative and the USAID Maternal and Child Survival Project. They have shared the design and start-up activities for the study at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. A summary follows:
Justin Tiendrebeogo, Ousmane Badolo, Mathurin Dodo, Danielle Burke, and Bill Brieger of Jhpiego have designed and are implementing a study to determine the effect of delivering Intermittent Preventive Treatment for Malaria in Pregnancy through community health workers in Burkina Faso with the support of the US President’s Malaria Initiative and the USAID Maternal and Child Survival Project. They have shared the design and start-up activities for the study at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. A summary follows:
CHW Flipchart Page
The Ministry of Health of Burkina Faso with the support of its partners initiated a study on the feasibility of increasing provision of Intermittent Preventive Malaria Treatment in pregnant women (IPTp) with sulfadoxine-pyrimethamine (SP) by involving existing community-based health workers (CBHWs). As Burkina Faso adopted the WHO recommendations for more doses of IPTp during pregnancy, it was proposed that the challenge of achieving coverage of third, fourth and additional doses could be met using CBHWs.
The approved protocol calls for CBHWs to refer pregnant women to antenatal care (ANC) to receive their first IPTp dose. Subsequent doses at one-month intervals would be provided by trained CBHWs, who would report back to supervising midwives at the ANC clinics. Several steps were taken to gain approval and set up the intervention.
CHW Using Flipchart
First, IPTp data from the health information system was gathered. IPTp coverage based on ANC registration in the 6 intervention clinics was 69% IPTp1, 68% IPTp2, 56% IPTP3, and 1% IPTp4. Similar information was obtained from the 6 control clinic catchment areas. Situation analysis found that while CBHW curriculum stresses the importance of ANC, it does not address IPTp at community level.
In response updated training materials have been developed. The study team also collected information on village size and availability of CBHWs, especially females. Among the villages in the catchment of the 6 intervention ANC clinics, 33 were found to lack female CBHWs.

Supervisory Meeting
As a result, the team needed to recruit additional female CBHWs, as revised national recruitment guidance stressed attainment of primary school certificate over gender, meaning mainly men had been hired previously. Two institutional review boards were involved and suggested the need to address the potential rare side effects of SP and concerns that community IPTp would not detract from ANC clinic attendance.
Since district and clinic level health staff will be involved in implementing the program using the national CBHW program, lessons learned from this effort to expand the work of CBHWs in preventing malaria in pregnancy should be applicable and adaptable to the whole country.
CHW &IPTp &Malaria in Pregnancy Bill Brieger | 05 Nov 2017
Improving Early ANC Attendance and IPT Uptake through Community Health Volunteers
 Community health workers are playing an increasing role in maternal health programming. Augustine Ngindu, Susan Ontiri, Gathari Ndirangu, Beth Barasa, Evans Nyapada, David Omoit, Johnstone Akatu, and Mildred Mudany of The Matewrnal and Child Survival Program, The Kenya Ministry of Health and Jhpiego share their experiences in Kenya at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Baltimore on 2017-11-06. If you are in Baltimore, hear more at Scientific Session 13. Below is an abstract of their presentation
Community health workers are playing an increasing role in maternal health programming. Augustine Ngindu, Susan Ontiri, Gathari Ndirangu, Beth Barasa, Evans Nyapada, David Omoit, Johnstone Akatu, and Mildred Mudany of The Matewrnal and Child Survival Program, The Kenya Ministry of Health and Jhpiego share their experiences in Kenya at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Baltimore on 2017-11-06. If you are in Baltimore, hear more at Scientific Session 13. Below is an abstract of their presentation
 Kenya adopted the use of intermittent preventive treatment with sulfadoxine pyrimethamine in 1998 but the proportion of pregnant women receiving at least two doses (22% (2010) and 56% (2015) has remained below the national target of 80%. In 2015, the country adopted an IPTp3 indicator for monitoring IPTp uptake; that year, the proportion of women taking at least 3 doses was 38% (2015).
Kenya adopted the use of intermittent preventive treatment with sulfadoxine pyrimethamine in 1998 but the proportion of pregnant women receiving at least two doses (22% (2010) and 56% (2015) has remained below the national target of 80%. In 2015, the country adopted an IPTp3 indicator for monitoring IPTp uptake; that year, the proportion of women taking at least 3 doses was 38% (2015).
Some of the factors leading to low IPTp coverage include poor knowledge on the need for early antenatal care (ANC), distances to health facilities, sociocultural practices and a lack of financial resources. In 2012, community health volunteers (CHVs) were enlisted through a pilot program in one county to deliver messages aimed at increasing the proportion of women starting ANC ? 20 weeks of gestation and thus expand the proportion of women receiving IPTp early in the second trimester.
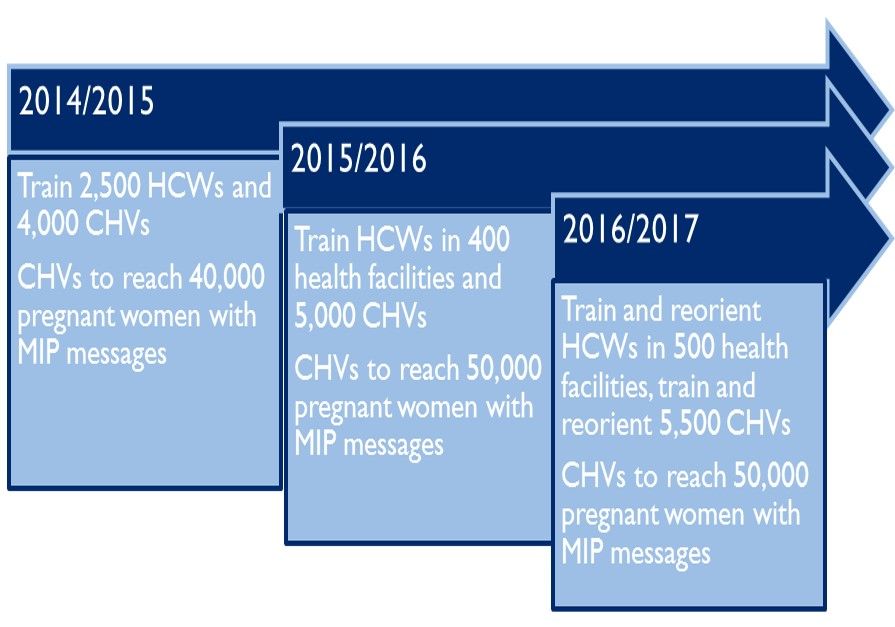
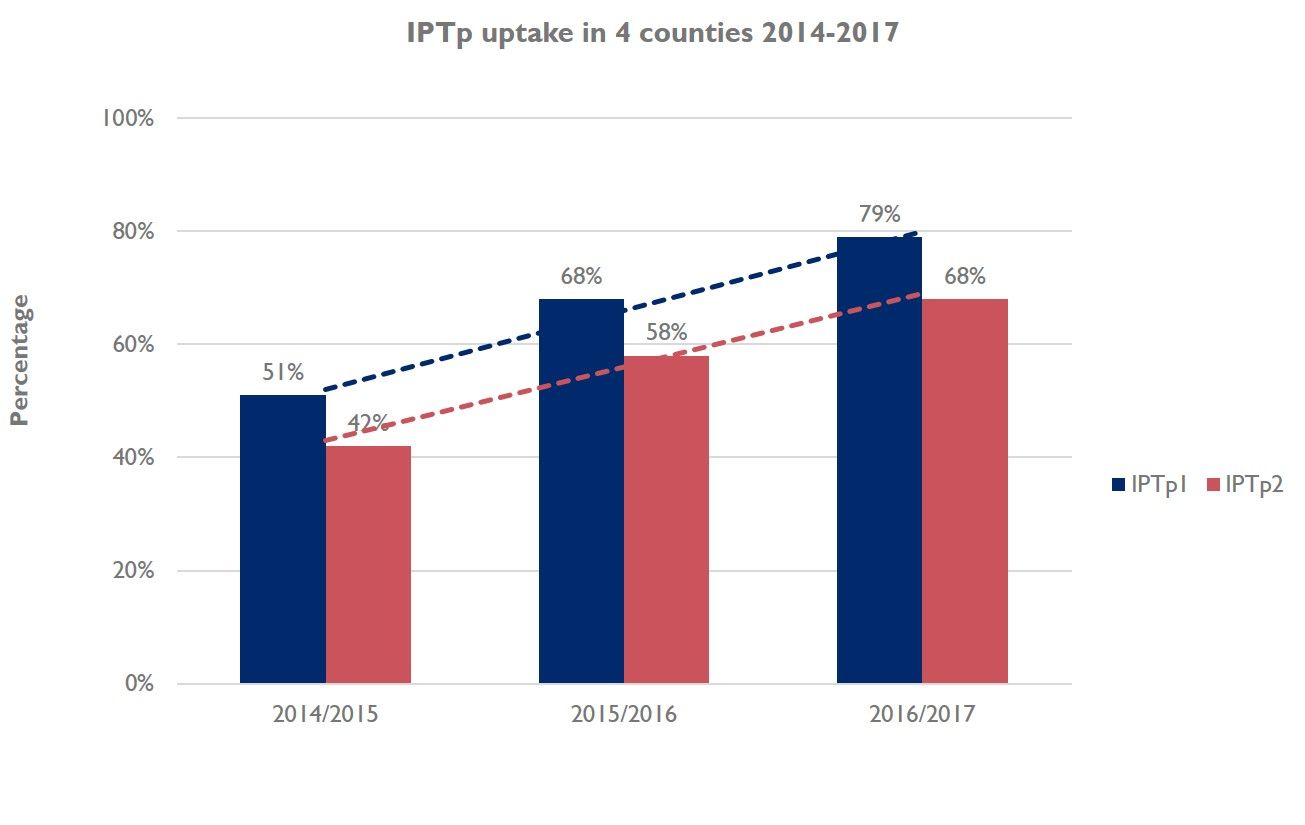 A community survey in 2013 showed an increase in IPTp2 from 22% in 2010 to 63%. The practice was considered a success story, and was subsequently replicated in 30 sub-counties, in 4 out of 14 malaria endemic counties. The rollout involved training of 9,042 CHVs, in 761 community units. Between 2015 and 2016, the CHVs reached 86,433 women with MiP messages. During this time, there was an average increase in IPTp1 from 51% to 68%, and IPTp2 increased from 42% to 55% (p? 0.001). This could be attributed to early ANC attendance, which increased from 32% to 48% in the same period.
A community survey in 2013 showed an increase in IPTp2 from 22% in 2010 to 63%. The practice was considered a success story, and was subsequently replicated in 30 sub-counties, in 4 out of 14 malaria endemic counties. The rollout involved training of 9,042 CHVs, in 761 community units. Between 2015 and 2016, the CHVs reached 86,433 women with MiP messages. During this time, there was an average increase in IPTp1 from 51% to 68%, and IPTp2 increased from 42% to 55% (p? 0.001). This could be attributed to early ANC attendance, which increased from 32% to 48% in the same period.
The use of CHVs to sensitize pregnant women to start IPTp early in the second trimester and continue with scheduled ANC visits increases the probability that women will receive the recommended IPTp-SP doses. The rollout of the practice to other malaria endemic counties is likely to have contributed to increase in IPTp uptake in the four target counties.
.![]()
Children &CHW &Human Resources &Mortality &Women Bill Brieger | 02 Aug 2017
Health for All at the International Institute for Primary Health Care, Ethiopia
 The time is ripe for a revitalization of the primary health care (PHC) movement. “Health for All through Primary Health Care” (HFA) was first envisioned at the 1978 International Conference on Primary Health Care (World Health Organization and UNICEF), and was enshrined in the Declaration of Alma-Ata. The HFA goal of bringing essential, affordable, scientifically sound, socially acceptable health care provided by health workers who are trained to work as a health team and who are responsive to the health needs of the community, guided by strong community engagement by the year 2000 but has not been fully met. Fortunately the vision of Alma-Ata has taken root, sprouted and flourished in a number of locations.
The time is ripe for a revitalization of the primary health care (PHC) movement. “Health for All through Primary Health Care” (HFA) was first envisioned at the 1978 International Conference on Primary Health Care (World Health Organization and UNICEF), and was enshrined in the Declaration of Alma-Ata. The HFA goal of bringing essential, affordable, scientifically sound, socially acceptable health care provided by health workers who are trained to work as a health team and who are responsive to the health needs of the community, guided by strong community engagement by the year 2000 but has not been fully met. Fortunately the vision of Alma-Ata has taken root, sprouted and flourished in a number of locations.
 Thanks to the vision and intellectual and political leadership of Dr. Tedros Adhanom Ghebreyesus, the then Minister of Health of Ethiopia and recently elected Director General of the World Health Organization, Ethiopia is an outstanding example of the Alma-Ata legacy. Access to PHC services was greatly expanded through the training of 40,000 Health Extension Workers (women from the local area with one year of training, each of whom serve 2,500 people and receive a government salary), recruitment of 3 million community female health volunteers (called the Health Development Army), and engagement with communities to enable them to take responsibility for improving their health.
Thanks to the vision and intellectual and political leadership of Dr. Tedros Adhanom Ghebreyesus, the then Minister of Health of Ethiopia and recently elected Director General of the World Health Organization, Ethiopia is an outstanding example of the Alma-Ata legacy. Access to PHC services was greatly expanded through the training of 40,000 Health Extension Workers (women from the local area with one year of training, each of whom serve 2,500 people and receive a government salary), recruitment of 3 million community female health volunteers (called the Health Development Army), and engagement with communities to enable them to take responsibility for improving their health.
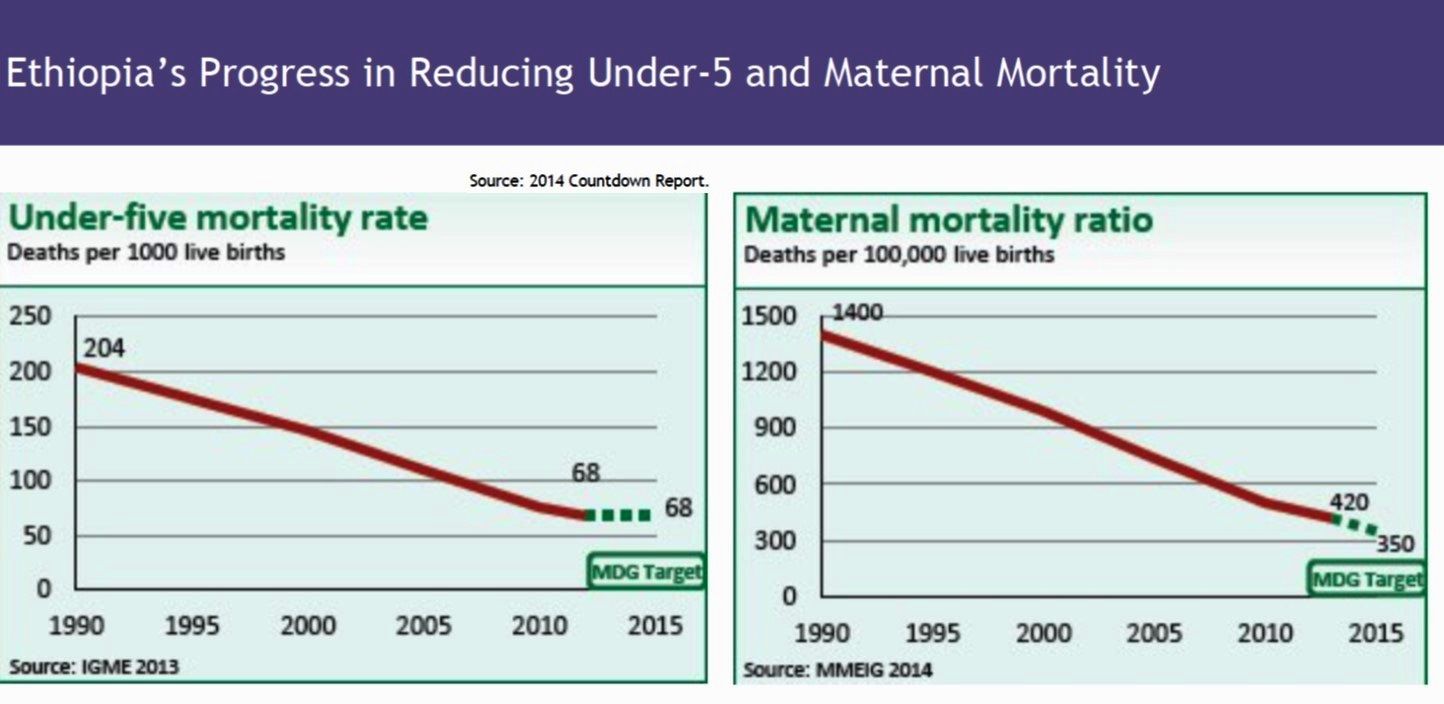
 This expansion of PHC enabled Ethiopia to achieve its health-related MDGs. Child mortality (those younger than 5 years of age) declined from 166 deaths per 1,000 live births in 1990 to 67 in 2016 (MDG 4). Significant progress was achieved in reducing levels of childhood malnutrition (MDG 1). MDG 5 was almost reached, with a decline in maternal morality of 72%, versus the goal of 75%, and the percentage of mothers obtaining a delivery by a skilled provider increased 6-fold between 1995 and 2016. The prevalence rate of modern contraceptive use increased from 6% in 2000 to 35% in 2016. MDG 6 (for HIV, malaria and tuberculosis) was also reached. The number of new HIV infections declined by 90%, and the number of AIDS-related deaths by 53%. Between 1990 and 2015, the tuberculosis incidence and mortality rate declined by 48% and 72%, respectively. The malaria incidence rate declined by 50% and malaria mortality by 60%. Ethiopia’s PHC system is acknowledged as the major factor leading to these impressive health gains.
This expansion of PHC enabled Ethiopia to achieve its health-related MDGs. Child mortality (those younger than 5 years of age) declined from 166 deaths per 1,000 live births in 1990 to 67 in 2016 (MDG 4). Significant progress was achieved in reducing levels of childhood malnutrition (MDG 1). MDG 5 was almost reached, with a decline in maternal morality of 72%, versus the goal of 75%, and the percentage of mothers obtaining a delivery by a skilled provider increased 6-fold between 1995 and 2016. The prevalence rate of modern contraceptive use increased from 6% in 2000 to 35% in 2016. MDG 6 (for HIV, malaria and tuberculosis) was also reached. The number of new HIV infections declined by 90%, and the number of AIDS-related deaths by 53%. Between 1990 and 2015, the tuberculosis incidence and mortality rate declined by 48% and 72%, respectively. The malaria incidence rate declined by 50% and malaria mortality by 60%. Ethiopia’s PHC system is acknowledged as the major factor leading to these impressive health gains.
 Representatives from more than half of sub-Saharan Africa countries have come to Ethiopia to see its PHC system in action. Because of this interest, in 2016 the Federal Ministry of Health of Ethiopia established the International Institute for Primary Health Care – Ethiopia, with seed funding from the Bill & Melinda Gates Foundation and technical support from the Johns Hopkins Bloomberg School of Public Health. Our goal is for the Institute to become a global center of excellence for training, knowledge dissemination and research in primary health care, supported by multiple donors.
Representatives from more than half of sub-Saharan Africa countries have come to Ethiopia to see its PHC system in action. Because of this interest, in 2016 the Federal Ministry of Health of Ethiopia established the International Institute for Primary Health Care – Ethiopia, with seed funding from the Bill & Melinda Gates Foundation and technical support from the Johns Hopkins Bloomberg School of Public Health. Our goal is for the Institute to become a global center of excellence for training, knowledge dissemination and research in primary health care, supported by multiple donors.
The Institute has begun to provide formalized short-term training to high-level policy makers and officials, program planners and managers, as well as to those engaged in service delivery, to see first-hand how an effective national PHC system functions. Trainees come from within Ethiopia and around the world. Trainees also visit communities, meet their leaders, and observe primary health care providers at work. Trainees will return to their home country with renewed energy and new vision and skills to revitalize their own primary health care system.
The Institute will also conduct and support research that yields evidence to guide ongoing strengthening of the Health Extension Program, and will rapidly disseminate open access information about recent advances in PHC. The Institute marks a significant step forward on the road to achieving the Alma-Ata vision of Health for All.
A website for IIfPHC-E is being built to provide further information about these programs and will be available at: www.iifphc.org.
This posting was prepared by: Kesetebirhan Admasu1, Michael J. Klag2, Yifru Berhan Mitke3, Amir Aman4, Mengesha Admassu5, Solomon Zewdu6, Jose Rimon7, Henry B. Perry8
1Chief Executive Officer, Rollback Malaria Partnership, Geneva, Switzerland and Chair, Advisory Board, International Institute for Primary Health Care — Ethiopia
2Dean, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
3Minister, Federal Ministry of Health, Government of Ethiopia, Addis Ababa, Ethiopia
4State Minister, Federal Ministry of Health, Government of Ethiopia, Addis Ababa, Ethiopia and Co-Chair, Advisory Board, International Institute for Primary Health Care – Ethiopia
5Executive Director, International Institute for Primary Health Care – Ethiopia, Addis Ababa, Ethiopia
6Health and Nutrition Development Lead – Ethiopia, Integrated Programs, Global Policy & Advocacy – Global Development, Bill& Melinda Gates Foundation, Addis Ababa, Ethiopia
7Director, Bill & Melinda Gates Institute for Population and Reproductive Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
8Coordinator for Johns Hopkins University Support of the International Institute for Primary Health Care – Ethiopia, Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
CHW &Community &IRS &Treatment Bill Brieger | 27 Apr 2017
Rwanda Celebrates World Malaria Day 2017 – community is a major focus
Dr. Noella Umulisa, the Malaria Team Lead or the USAID Maternal and Child Survival Program in Kigali Rwanda shares with us experiences from Rwanda’s recent observance of World Malaria Day 2017.
The Malaria Day celebration took place in Huye districts in the southern Province. Why the southern province? – because among the 10 high endemic districts, 6 are the southern province. Why Huye district? – because IRS has been launched in Huye district yesterday and in another district Nyanza in Southern province.
 The ceremony was attended by USAID and WHO representative, local leaders, MOH staff, partners, population of Simbi sector and the guest of honour was Dr Jeannine Condo the Director General of Rwanda Biomedical Center (which houses malaria activities).
The ceremony was attended by USAID and WHO representative, local leaders, MOH staff, partners, population of Simbi sector and the guest of honour was Dr Jeannine Condo the Director General of Rwanda Biomedical Center (which houses malaria activities).
A special recognition was given to community health workers (CHWs) who are playing a key role and are on the front line of fighting Malaria through sensitization of the population, testing and treating the population through community case management (iCMM and HBM) of Malaria, and now when a big number of CHWs will be involved in spraying households in their community.
 The World Malaria Day celebration in Rwanda is marked by different activities for Malaria prevention conducted at community level from 24th to 29th April 2017. Also, Malaria prevention and control messages are being disseminated using different communication tools and approaches such as radio and TV programs, community outreach activities, educating communities on proper use of bed nets.
The World Malaria Day celebration in Rwanda is marked by different activities for Malaria prevention conducted at community level from 24th to 29th April 2017. Also, Malaria prevention and control messages are being disseminated using different communication tools and approaches such as radio and TV programs, community outreach activities, educating communities on proper use of bed nets.
Door to door mobilization is being conducted about the Indoor Residual Spraying (IRS) in high malaria burden districts of Huye and Nyanza. MCSP, with support from the US President’s Malaria Initiative, has participated actively in this event by supporting Community outreaches though theatre skits in the first 10 high endemic district.
 The Director General made the following statement:
The Director General made the following statement:
In January 2016, the Government of Rwanda and partners developed a Malaria Contingency Plan in response to the increase in malaria cases. The following interventions were implemented to address malaria rise in Rwanda: A Home Based Management of fever for adults at community level was set up countywide to reduce the malaria burden and prevent severe malaria and death. From Nov 2016 up to March 2017, the country distributed more than 6 million nets in 30 districts ensuring universal coverage of the entire population.
The country has increased access to health services for all through Community Based Health Insurance (CBHI). The Government of Rwanda provides free treatment of malaria to the most vulnerable population (Ubudehe 1&2 categories) to ensure that all financial barriers are no more to hinder the health service delivery for the community. Extension of Indoor residual spraying (IRS) in districts with high malaria burden where 5 out of 8 were sprayed (Nyagatare, Kirehe, Bugesera, Gisagara and Gatsibo).
We hope that this commitment will keep Rwanda on track to control and eventually eliminate malaria.
CHW &Community Bill Brieger | 12 Apr 2017
Success Stories in Community Health in Africa
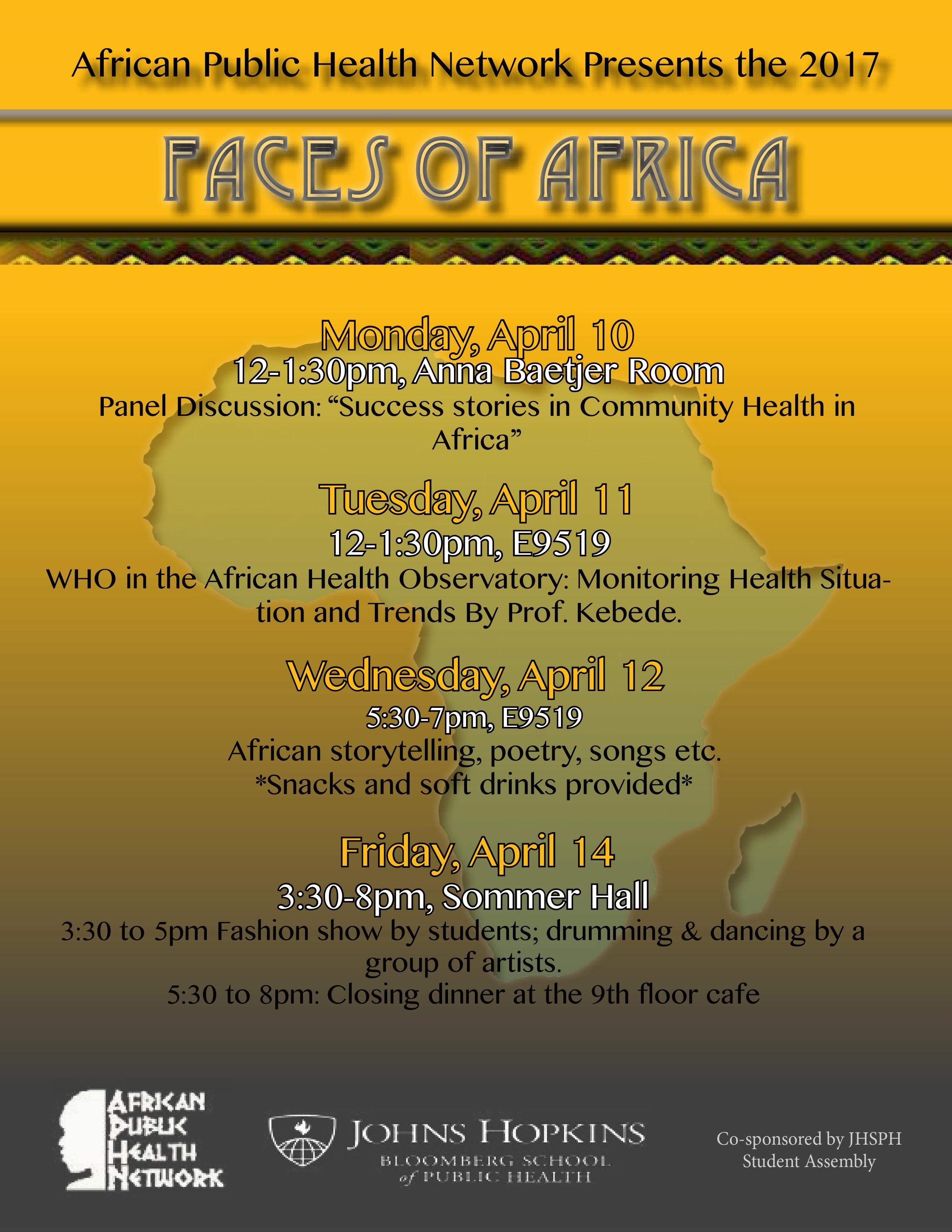 The African Public Health Network of the Johns Hopkins Bloomberg School of Public Health held a panel discussion about community health successes in Africa on Monday 10th of April as the first in a series of events for the annual “Faces of Africa Week”.
The African Public Health Network of the Johns Hopkins Bloomberg School of Public Health held a panel discussion about community health successes in Africa on Monday 10th of April as the first in a series of events for the annual “Faces of Africa Week”.
Africa evokes different reactions to different people. For many, it’s the pictures of starving children, wars, poverty and disease that they find in various print and electronic media. But there has been a lot of achievement in Africa!
The Johns Hopkins Bloomberg School of Public Health – an institution that has invested a lot of time and resources in saving millions of lives at a time- has a huge footprint on the continent and other parts of the developing world through the work done and being done by experienced faculty members. Here is a summary of there thoughts as presented at Monday’s panel.
 Dr. Henry Perry led the panel discussion on ‘The success stories in Public Health in Africa in the context of the role of Community Based Health Care’. He provided insights from the experiences of Rwanda and Ethiopia. He stressed the achievements of both countries in establishing and scaling up community health worker programs and in achieving Millennium Development Goals with reduced child mortality.
Dr. Henry Perry led the panel discussion on ‘The success stories in Public Health in Africa in the context of the role of Community Based Health Care’. He provided insights from the experiences of Rwanda and Ethiopia. He stressed the achievements of both countries in establishing and scaling up community health worker programs and in achieving Millennium Development Goals with reduced child mortality.
 Dr. William Brieger shared his experience from having lived and worked in Nigeria for over 27 years. He shared the progress in working with volunteer health workers and helping to shape community directed interventions. This history ranged from volunteer CHW programs by local NGOs, FBOs and universities in the 1970s to the development of a standardized set of CHW guidance and training materials by the Federal Ministry of Health in 2012. In the 1990s Nigeria took part in WHO’s African Program for Onchocerciasis Control and established a system of community directed treatment with ivermectin (CDTI) and community directed distributors to enable communities to take charge of annual ivermectin delivery. Then in the 2000s efforts build on the CDTI model to create the community directed intervention approach that included delivery of malaria
Dr. William Brieger shared his experience from having lived and worked in Nigeria for over 27 years. He shared the progress in working with volunteer health workers and helping to shape community directed interventions. This history ranged from volunteer CHW programs by local NGOs, FBOs and universities in the 1970s to the development of a standardized set of CHW guidance and training materials by the Federal Ministry of Health in 2012. In the 1990s Nigeria took part in WHO’s African Program for Onchocerciasis Control and established a system of community directed treatment with ivermectin (CDTI) and community directed distributors to enable communities to take charge of annual ivermectin delivery. Then in the 2000s efforts build on the CDTI model to create the community directed intervention approach that included delivery of malaria  services (ITNs, Case management and intermittent preventive treatment), vitamin A and DOTS for TB through community effort.
services (ITNs, Case management and intermittent preventive treatment), vitamin A and DOTS for TB through community effort.
Dr. Anbrasi Edward shared the Mozambique experience highlighting the Vurhonga projects and the impact of the care group model in improving maternal and child health. She described how the Care Group model was developed by an NGO that involved community volunteers providing education and services to small groups of community members. This model has spread throughout Africa.
 Mr. Bonny Musefano from the Embassy of The Republic of Rwanda provide perspectives on how Rwanda rebuilt its health system after the 1994 genocide ultimately leading to good community health. He stress the importance of Rwanda’s innovative system of community health insurance called Mutuelles de Santé. Very high coverage means that almost all Rwandans have access to health care. He also stressed the country’s interest in innovative technology and how drones are being used to deliver medical supplies to remote areas.
Mr. Bonny Musefano from the Embassy of The Republic of Rwanda provide perspectives on how Rwanda rebuilt its health system after the 1994 genocide ultimately leading to good community health. He stress the importance of Rwanda’s innovative system of community health insurance called Mutuelles de Santé. Very high coverage means that almost all Rwandans have access to health care. He also stressed the country’s interest in innovative technology and how drones are being used to deliver medical supplies to remote areas.
The APHN is grateful to members of the panel and to Prof. David Peters who helped fund the event via the Department of International Health.
For APHN: Joseph Uwazota, Jean Olivier Twahirwa Rwema, Zyleen Kassamali, Eve-Marie Benson, and Massah Massaquoi
CHW &Diagnosis &Health Workers &Performance &Training &Treatment Bill Brieger | 06 Apr 2017
World Health Workers Week, a Time to Recognize Health Worker Contributions to Malaria Care
 Since the beginning of the Roll Back malaria Partnership in 1998 there has been strong awareness that malaria control success is inextricably tied to the quality of health systems. Achieving coverage of malaria interventions involves all aspects of the health system but most particularly the human resources who plan, deliver and assess these services. World Health Worker Week is a good opportunity to recognize health worker contributions to ridding the world of malaria.
Since the beginning of the Roll Back malaria Partnership in 1998 there has been strong awareness that malaria control success is inextricably tied to the quality of health systems. Achieving coverage of malaria interventions involves all aspects of the health system but most particularly the human resources who plan, deliver and assess these services. World Health Worker Week is a good opportunity to recognize health worker contributions to ridding the world of malaria.
We can start with community health workers who may be informal but trained volunteers or front line formal health staff. According to the Frontline Health Workers Coalition, “Frontline health workers provide immunizations and treat common infections. They are on the frontlines of battling deadly diseases like Ebola and HIV/AIDS, and many families rely on them as trusted sources of information for preventing, treating and managing a variety of leading killers including diarrhea, pneumonia, malaria and tuberculosis.”
 The presence of CHWs exemplifies the ideal of a partnership between communities and the health system. With appropriate training and supervision CHWs ensure that malaria cases are diagnosed and treated promptly and appropriately, malaria prevention activities like long lasting insecticide-treated nets are implemented and pregnant women are protected from the dangers of the disease. CHWs save lives according to Nkonki and colleagues who “found evidence of cost-effectiveness of community health worker (CHW) interventions in reducing malaria and asthma, decreasing mortality of neonates and children, improving maternal health, increasing exclusive breastfeeding and improving malnutrition, and positively impacting physical health and psychomotor development amongst children.”
The presence of CHWs exemplifies the ideal of a partnership between communities and the health system. With appropriate training and supervision CHWs ensure that malaria cases are diagnosed and treated promptly and appropriately, malaria prevention activities like long lasting insecticide-treated nets are implemented and pregnant women are protected from the dangers of the disease. CHWs save lives according to Nkonki and colleagues who “found evidence of cost-effectiveness of community health worker (CHW) interventions in reducing malaria and asthma, decreasing mortality of neonates and children, improving maternal health, increasing exclusive breastfeeding and improving malnutrition, and positively impacting physical health and psychomotor development amongst children.”
 CHWs do not act in isolation but depend on health workers at the facility and district levels for training, supervision and maintenance of supplies and inventories. These health staff benefit from capacity building – when they are capable of performing malaria tasks, they can better help others learn and practice.
CHWs do not act in isolation but depend on health workers at the facility and district levels for training, supervision and maintenance of supplies and inventories. These health staff benefit from capacity building – when they are capable of performing malaria tasks, they can better help others learn and practice.
A good example of this capacity building is the Improving Malaria Care (IMC) project in Burkina Faso, implemented by Jhpiego and supported by USAID and the US President’s malaria Initiative. IMC builds capacity of health workers at facility and district level to improve malaria prevention service delivery and enhance accuracy in malaria diagnosis and treatment. Additionally capacity building is provided to health staff in the National Malaria Control Program to plan, design, manage and coordinate a comprehensive malaria control program. As a result of capacity building there has been a large increase in malaria cases diagnosed using parasitological techniques and in the number of women getting more doses of intermittent preventive treatment to prevent malaria during pregnancy.
Malaria care is much more than drugs, tests and nets. Health worker capacity is required to get the job done and move us forward on the pathway to eliminate malaria.