IPTp &Malaria in Pregnancy &Private Sector Bill Brieger | 04 Nov 2014 06:52 am
A role for the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya
Jhpiego staff will again present a poster at the Tuesday noon (Nov 4) session of the American Society of Tropical Medicine and Hygiene Annual Meeting. Augustine M. Ngindu, Muthoni M. Kariuki, Sanyu Kigondu, Johnstone Akatu, Isaac M. Malonza, with support from USAID’s Maternal and Child Health Integrated Project (MCHIP) will share experiences with a poster titled, “Improving maternal and neonatal health: Complementary role of the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya.” The abstract is provided below.
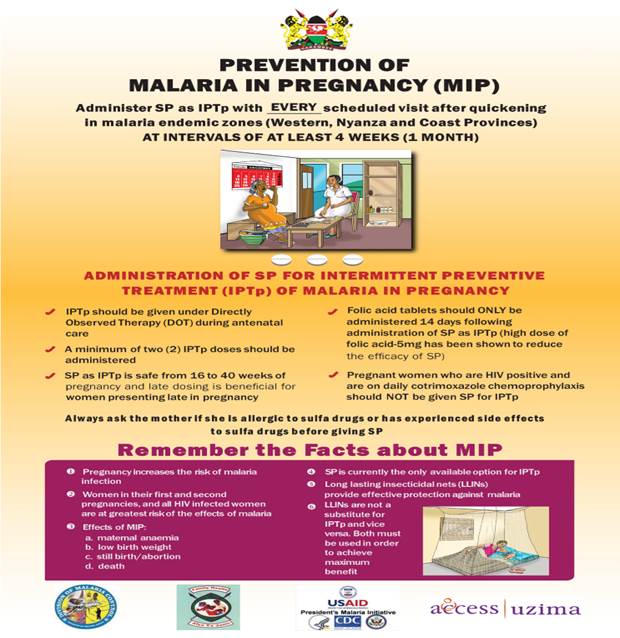
 Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
To increase the coverage rate, MCHIP supported malaria control and reproductive health divisions of the ministry of health, first to harmonize knowledge among service providers on provision of IPTp-SP in 2011, and second to train community health workers (CHWs) on sensitization of pregnant women to start early antenatal care (ANC) attendance in 2012.
 A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A total of 15 (58%) out all 26 health facilities in the sub-county (public – 6 out of 8, faith-based – 2 out 3 and private – 7 out of 15) were selected. Data on new ANC clients, revisits and IPTp doses given was collected from the ANC registers.
Among th e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
In 2013 the government declared provision of free maternity services in public facilities but ANC clients have continued to utilize services from the private sector. This is an indication of the untapped potential in the private sector in increasing access to high impact interventions and importance of supporting the sector by all partners to provide these interventions.
Such complementary efforts if implemented will not only result in enabling the country to move towards achievement of set targets but also improve pregnancy outcomes through reduction in effects of
malaria in pregnancy.