CHW &Integration &IPTi &IPTp &Malaria in Pregnancy &Maternal Health &Seasonal Malaria Chemoprevention Bill Brieger | 12 Dec 2022
Malaria Chemoprevention in 2021 as Seen in The World Malaria Report of 2022
 Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, reminds us in this year’s edition of the World Malaria Report (WMR 2022) that, “Although hard hit, most countries held the line and were able to maintain services to prevent, detect and treat malaria – a remarkable feat in the midst of a pandemic. Nonetheless, more than 600 000 people still die of malaria every year – most of them children. Even with the heroic efforts to maintain services during the pandemic, malaria control efforts face many hurdles in addition to the already significant COVID-related disruptions and other health system challenges.”
Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, reminds us in this year’s edition of the World Malaria Report (WMR 2022) that, “Although hard hit, most countries held the line and were able to maintain services to prevent, detect and treat malaria – a remarkable feat in the midst of a pandemic. Nonetheless, more than 600 000 people still die of malaria every year – most of them children. Even with the heroic efforts to maintain services during the pandemic, malaria control efforts face many hurdles in addition to the already significant COVID-related disruptions and other health system challenges.”
Even though there was an increase in cases between 2020 and 2021, there are now more strategies in the malaria control and elimination toolkit than ever before. One in particular is an updated take on an old concept of chemoprophylaxis, which fell out of use due to mounting drug resistance. Years of research with pregnant women and young children led to the development over time of using regularly scheduled treatment doses of malaria medicines as chemoprevention. Intermittent Preventive Treatment for pregnant women (IPTp) and Seasonal Malaria Chemoprevention for young children, both targeted to appropriate epidemiological settings, are now common. Countries are also exploring IPT for children in other settings.
 We were, therefore, curious what the current WMR shares on chemoprevention initiatives. Specifically, the WMR summarized WHO recommendations as follows: “Updated guidelines provide recommendations on intermittent preventive treatment of malaria in pregnancy (IPTp), perennial malaria chemoprevention (PMC) and seasonal malaria chemoprevention (SMC), intermittent preventive treatment of malaria in school-aged children (IPTsc), post-discharge malaria chemoprevention (PDMC), mass drug administration (MDA) and elimination.”
We were, therefore, curious what the current WMR shares on chemoprevention initiatives. Specifically, the WMR summarized WHO recommendations as follows: “Updated guidelines provide recommendations on intermittent preventive treatment of malaria in pregnancy (IPTp), perennial malaria chemoprevention (PMC) and seasonal malaria chemoprevention (SMC), intermittent preventive treatment of malaria in school-aged children (IPTsc), post-discharge malaria chemoprevention (PDMC), mass drug administration (MDA) and elimination.”
In summary, WMR 2022 notes that, “The average number of children treated per cycle of SMC increased from about 0.2 million in 2012 to almost 45 million in 2021,” and “Using data from 33 countries in the WHO African Region, the percentage of IPTp use by dose was computed. In 2021, 72% of pregnant women used ANC services at least once during their pregnancy. About 55% of pregnant women received one dose of IPTp, 45% received two doses and 35% received three doses.” This is not just progress over time, but also represents an expansion targets and work required for success. For pregnant women the increase represented a change in target from only two doses during pregnancy to a minimum of three. Starting with pilot efforts, SMC now covers children in 15 countries.
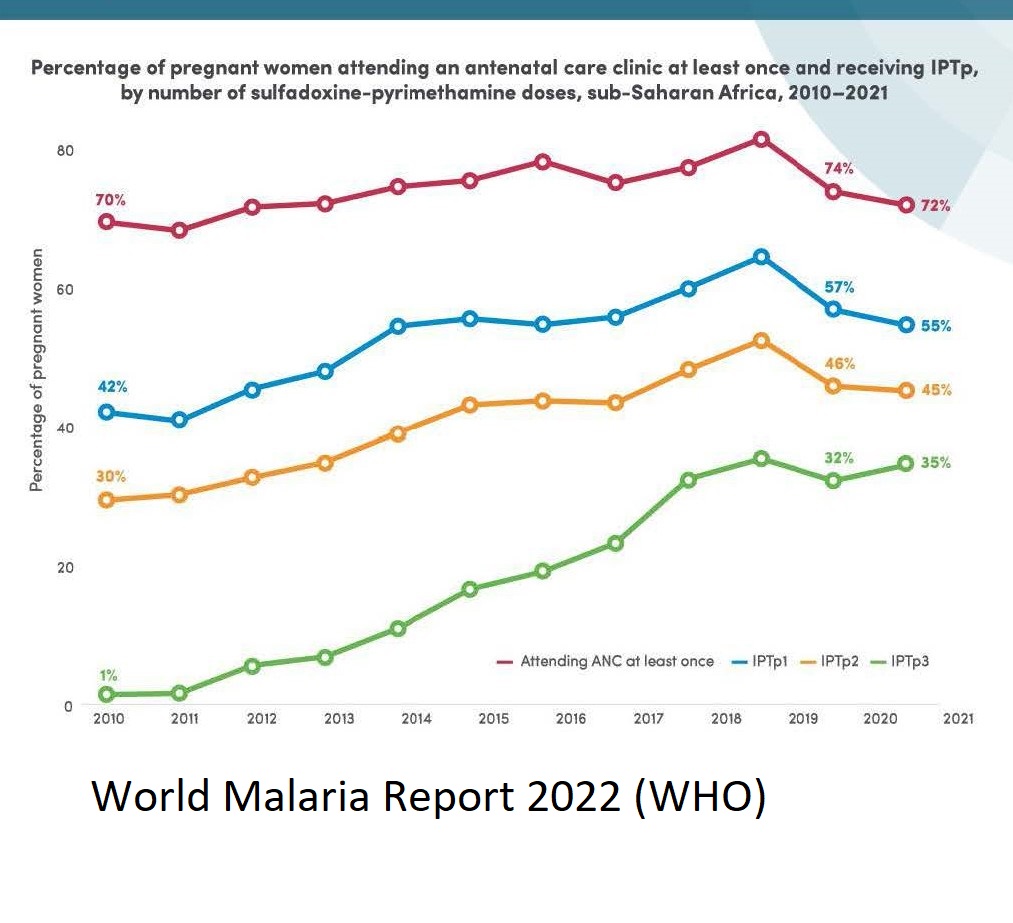 The targeted three doses for IPTp shows that two thirds of women who register for antenatal (prenatal) care (ANC), fail to achieve full coverage. Stronger collaboration is needed between malaria control and maternal health programs to ensure that pregnant women actually attend ANC and do so early and often enough to receive 3 monthly doses minimum in their second and third trimesters. More emphasis is needed on community IPTp distribution, since we know that community health workers have been crucial in achieving SMC as well as integrated community case management efforts.
The targeted three doses for IPTp shows that two thirds of women who register for antenatal (prenatal) care (ANC), fail to achieve full coverage. Stronger collaboration is needed between malaria control and maternal health programs to ensure that pregnant women actually attend ANC and do so early and often enough to receive 3 monthly doses minimum in their second and third trimesters. More emphasis is needed on community IPTp distribution, since we know that community health workers have been crucial in achieving SMC as well as integrated community case management efforts.
Similar challenges exist for SMC as research looks into whether additional doses are needed based on mosquito breeding and malaria transmission season factors in endemic countries. Adding extra months to the program will tax resources, but also save lives.
Both maternal and child efforts at chemoprevention will need to address research that first shows increasing resistance to the common medicines used, and the potential for introducing new drug combinations in light of that resistance. Challenges here reflect another aspect of SMC, the need for CHWs to guarantee that on any given distribution round, three doses on medicine are required. Recent reports show that within any given round, community adherence to SMC has been good. We need to apply those lessons to IPTp when the regimen changes.
Ultimately, chemoprevention has proven to be an important life saving tool. The challenges of multiple contacts and doses that lead to success rely not only on having effective medicines, but also on culturally appropriate behavior change strategies and well-funded efforts to strengthen the health systems that deliver preventive treatments.
Capacity Building &Conflict &Health Systems &Integration Bill Brieger | 07 Sep 2020
Malaria News Today 2020-09-07
Today’s updates are brief and look at Vietnam in Southeast Asia and South Sudan in Africa. Both are concerned with health systems issues. Please click on links to read more details.
Malaria Week 2020 – Why Integration Could Be the Key to Elimination
Hosted by the Government of Vietnam, Malaria Week 2020 (7-11 September) brings together government officials and diverse partners to drive forward the elimination of malaria from Asia Pacific by 2030. This year’s theme centres on the three I’s – Inclusion. Integration. Innovation – and captures the ambition to unite the region and harness innovation as efforts intensify to eradicate malaria globally and in Asia Pacific. Key topics in the series this week include surveillance systems, sustaining health financing, and innovation within the malaria landscape.
Given the backdrop of COVID-19 to this year’s event, discussions will have a focus on sustaining health financing and in particular malaria interventions during a pandemic, the critical role of community-based approaches in health systems strengthening and the need for strong surveillance and timely reporting, in addition to the role of innovation and private provider engagement in accelerating malaria elimination and strengthening health security.
Healthcare in South Sudan: A Fractured System
A limited access to healthcare facilities, medical supplies in South Sudan results in high number of preventable deaths. high rates of tuberculosis, HIV/AIDS, malaria, and diarrheal diseases in country.
The South Sudanese population has very limited access to healthcare facilities, with only 44% of the population living within a one-hour walk of a medical center. This adds an extra burden on those in need of medical attention as the majority of the population has to walk for an extended time to reach a medical center. During a time of civil unrest, traveling for an extended period comes with increased exposure to the risk of ambushes and looting.
Community &COVID-19 &Dracunculiasis Guinea Worm &Elimination &Integration &NTDs &Snakebite &Surveillance Bill Brieger | 19 May 2020
Tropical Diseases and the World Health Assembly 73rd Meeting
If it were not difficult enough to guide global health during a pandemic, some world leaders are trying to deflect attention from the real dangers at hand to score on their petty political concerns. In the meantime, we need to focus on what tropical health and disease issues may actually be coming under consideration at the virtual WHA 73.
 Agenda item 3 (A73/CONF./1 Rev.1) or “COVID-19 response Draft resolution” directly addresses the concerns of many that other major deadly diseases and essential services should not be further neglected. The large group of resolution proponents urge countries and organizations to,
Agenda item 3 (A73/CONF./1 Rev.1) or “COVID-19 response Draft resolution” directly addresses the concerns of many that other major deadly diseases and essential services should not be further neglected. The large group of resolution proponents urge countries and organizations to,
“Maintain the continued functioning of the health system in all relevant aspects, in accordance with national context and priorities, necessary for an effective public health response to the COVID-19 pandemic and other ongoing epidemics, and the uninterrupted and safe provision of population and individual level services, for, among others, communicable diseases, including by undisrupted vaccination programmes, neglected tropical diseases, noncommunicable diseases, mental health, mother and child health and sexual and reproductive health and promote improved nutrition for women and children, recognizing in this regard the importance of increased domestic financing and development assistance where needed in the context of achieving UHC.”
In Provisional agenda item 23 (A73/32) “Progress reports by the Director-General” we find updates on guinea worm eradication and the burden of snakebite envenoming. The report notes the situation in 2019, which is a far cry from the millions of cases in the 1980d when the dracunculiasis eradication effort was launched. “In 2019, three countries reported a total of 53 human indigenous cases of dracunculiasis (guinea-worm disease), namely, Angola (one case), Chad (48 cases) and South Sudan (four cases), from a total of 28 villages. Cameroon reported one human case, probably imported from Chad.”
It is important to note that, “The global dracunculiasis eradication campaign is based on both community and country-focused interventions,” where community members play an important role in surveillance and notification. This includes at-risk and border areas, as is being done in Cameroon. The challenge of human Dracunculus medinensis infection in dogs continues and points to the importance of One Health in the control and elimination of NTDs. Surveillance is not cheap, and the report stresses that funds are still needed so that international partners can continue to ensure that the last case of guinea worm is detected and contained.
Moving from the smaller serpent to the larger variety, the report recalls the May 2018 World Health Assembly resolution WHA71.5 on addressing the burden of snakebite envenoming. A global strategy, “Snakebite envenoming: a strategy for prevention and control” was launched in in May 2019. The WHO Secretariat has “fostered international efforts to improve the availability, accessibility and affordability of safe and effective antivenoms for all, through assessments of antivenom manufacturing, training programs and stockpile procedures.
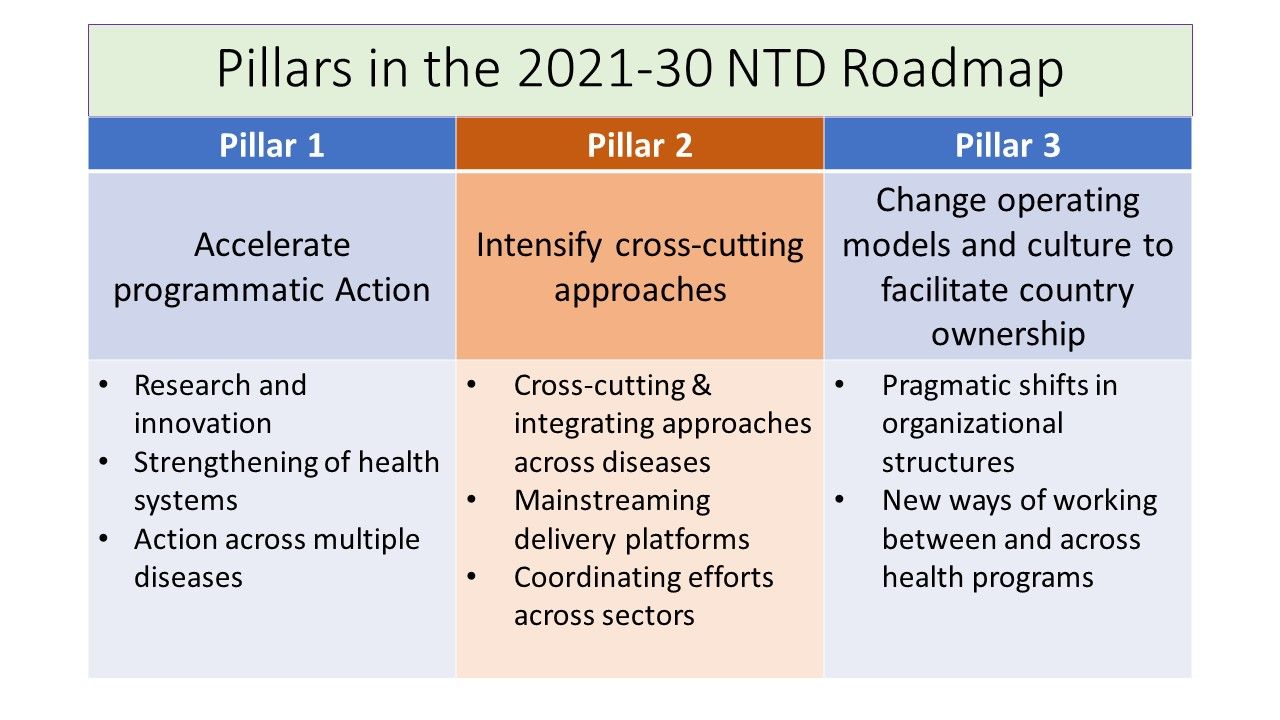 Finally, provisional agenda item 11.8 (A73/8) addresses a “Draft road map for neglected tropical diseases 2021–2030.” This builds on resolution WHA66.12 (2013) on WHO’s earlier road map for accelerating work to overcome the global impact of neglected tropical diseases (2012–2020). The proposed interventions build on important principles including:
Finally, provisional agenda item 11.8 (A73/8) addresses a “Draft road map for neglected tropical diseases 2021–2030.” This builds on resolution WHA66.12 (2013) on WHO’s earlier road map for accelerating work to overcome the global impact of neglected tropical diseases (2012–2020). The proposed interventions build on important principles including:
- Tackling neglected tropical diseases through support of the vision of universal health coverage
- Adopting grassroots approaches that enable access to some of the world’s poorest, hard-to reach communities and people affected by complex emergencies
- Monitoring progress against neglected tropical diseases as a litmus test of progress towards the achievement of universal health coverage
The report notes that “40 countries, territories and areas have eliminated at least one neglected tropical disease,” most notably dracunculiasis (as mentioned above, lymphatic filariasis and trachoma. Although “substantive progress has been made since 2012, it is evident that not all of the 2020 targets will be met.” Hence, a new draft road map for neglected tropical diseases for 2021–2030 is required. The three pillars supporting the new roadmap are outlined in the attached figure.
It is good to know that the 73rd World Health Assembly will not be completely overshadowed by COVID-19 and politics. Efforts to sustain and improve NTD control and elimination must not be jeopardized.
Integration &NTDs Bill Brieger | 18 Jun 2018
Milestones in Eliminating NTDs
WHO lists the milestones towards validation of elimination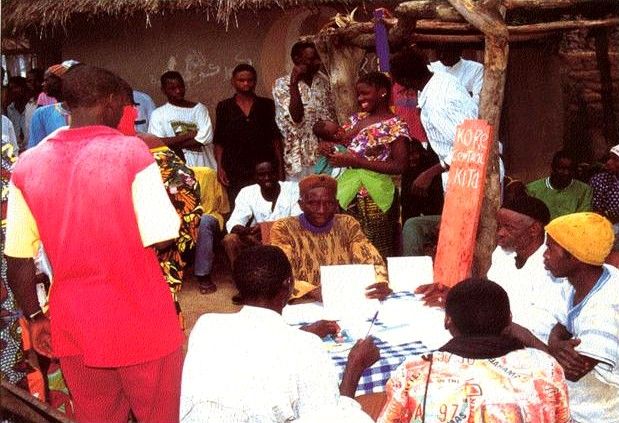 beginning with stopping the spread of infection through mass drug administration (MDA), implementing MDA in all endemic areas (100% geographical coverage), reducing infection below a threshold at which transmission is not sustainable in all endemic areas and stop MDA, and finally demonstrating sustained reduction of infection below the threshold no earlier than 4 years after stopping MDA. WHO also encourages countries to alleviate suffering by managing morbidity such as lymphedema and preventing disability.
beginning with stopping the spread of infection through mass drug administration (MDA), implementing MDA in all endemic areas (100% geographical coverage), reducing infection below a threshold at which transmission is not sustainable in all endemic areas and stop MDA, and finally demonstrating sustained reduction of infection below the threshold no earlier than 4 years after stopping MDA. WHO also encourages countries to alleviate suffering by managing morbidity such as lymphedema and preventing disability.
By 2015 the partners providing PCT achieved a milestone. As WHO reports, “Preventive chemotherapy is achievable, as proven by the increasing numbers of people being reached each year. In 2015, over 1.5 billion treatments were administered to almost 1 billion individuals for at least one of the targeted infections: lymphatic filariasis, onchocerciasis, schistosomiasis soil-transmitted helminthiases and trachoma.

village records of MDA activities
At a low cost – between US$ 0.30 and US$ 0.50 per person treated in most settings – preventive chemotherapy remains the most affordable, cost-effective strategy for controlling and eliminating these diseases.” WHO also explains that to be fully sustainable and to maximize impact, PCT the strategy should be combined and delivered with other interventions, including improving access to safe drinking-water, hygiene, disease management and vector control.
USAID as one of the major NTD partners has spent nearly $700 million since 2006 to build the capacity of 33 endemic countries to plan and implement the MDA strategy for the five PCT diseases. By 2016, “USAID-assisted NTD programs had provided a total of more than 2 billion treatments in the respective countries, representing 935 million persons treated.” Over these years the number of persons living in implementation units (e.g. districts) that no longer require MDA has steadily increased.
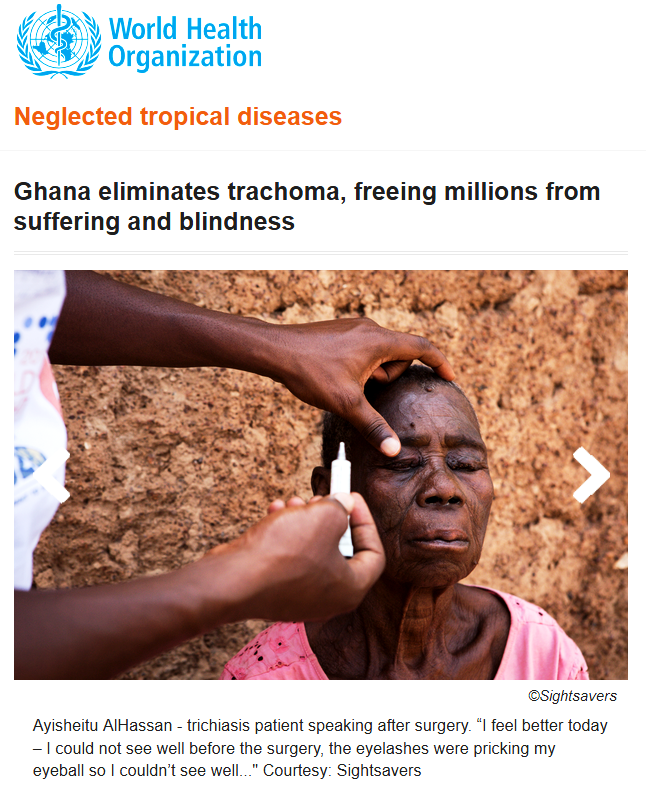 Of the 25 countries USAID has supported for LF MDA, “Three had already stopped MDA treatment in 2015 (Togo, Cambodia, and Vietnam), Four were expected to stop MDA in 2017, and 10 more countries by 2020. There were eight countries where the date for stopping treatment was anticipated beyond 2020.” Likewise, “Most countries are on track to reach WHO 2020 elimination goals for trachoma,” and nearly all countries shown anticipate reaching post-MDA surveillance by 2021.
Of the 25 countries USAID has supported for LF MDA, “Three had already stopped MDA treatment in 2015 (Togo, Cambodia, and Vietnam), Four were expected to stop MDA in 2017, and 10 more countries by 2020. There were eight countries where the date for stopping treatment was anticipated beyond 2020.” Likewise, “Most countries are on track to reach WHO 2020 elimination goals for trachoma,” and nearly all countries shown anticipate reaching post-MDA surveillance by 2021.
In conclusion, Robollo and Bockarie remind us that, “Interventions against neglected tropical diseases (NTD), including lymphatic filariasis (LF), (were) scaled up dramatically after the signing of the London Declaration (LD) in 2012… but some countries are considered not on track to meet the 2020 target using the recommended preventive chemotherapy and morbidity management strategies.” They believe that LF can be eliminated by 2020 “using cross-sectoral and integrated approaches” that incorporate the synergistic effect of the Sustainable Development Goals related to poverty reduction and water and sanitation.
Integration &NTDs &Tuberculosis Bill Brieger | 24 Mar 2017
World Tuberculosis Day: United We Can End TB and Tropical Diseases
 The theme of World TB Day is to Unite to end TB: leave no one behind. The communities affected by TB are also ones where tropical diseases like onchocerciasis and malaria are endemic. A successful strategy to control one disease should ideally be “united” with all basic primary health care interventions, thereby truly leaving no one behind.
The theme of World TB Day is to Unite to end TB: leave no one behind. The communities affected by TB are also ones where tropical diseases like onchocerciasis and malaria are endemic. A successful strategy to control one disease should ideally be “united” with all basic primary health care interventions, thereby truly leaving no one behind.
While the causative agents differ between TB and tropical diseases such as malaria, lymphatic filariasis and Dengue, control of these diseases shares a common goal – “an urgent need to develop new vaccines for HIV/AIDS, malaria, and tuberculosis, as well as for respiratory syncytial virus and those chronic and debilitating (mostly parasitic) infections known as neglected tropical diseases (NTDs).” In addition to prevention, there is also need for integrated “treatment pipelines directed at NTDs, Malaria, tuberculosis (TB), and human immunodeficiency virus (HIV)/AIDS,” according to Asada.
There is also a need for integrated primary health care (PHC) programming. In the Journal of Infectious Diseases. Simon reports on linkages showing that, “Recent research suggests that NTDs can affect HIV and AIDS, tuberculosis (TB), and malaria disease progression. A combination of immunological, epidemiological, and clinical factors can contribute to these interactions and add to a worsening prognosis for people affected by HIV/AIDS, TB, and malaria.”
 The possibility of integrating directly observed treatment (DOT) for TB treatment into community health worker (CHW)/PHC programs that addressed malaria treatment and onchocerciasis control was tested by the Tropical Disease Research Program (TDR) some years ago. CHWs in a few of the study sites were able to successfully include DOT for TB in their community duties, but in other sites community and health worker fears about stigma inhibited action.
The possibility of integrating directly observed treatment (DOT) for TB treatment into community health worker (CHW)/PHC programs that addressed malaria treatment and onchocerciasis control was tested by the Tropical Disease Research Program (TDR) some years ago. CHWs in a few of the study sites were able to successfully include DOT for TB in their community duties, but in other sites community and health worker fears about stigma inhibited action.
TB, malaria and NTDs are among the conditions referred to as the infectious diseases of poverty. We will not eliminate poverty by tackling these diseases one-by-one. A “United” and integrated approach from national to community level is needed.
Integration &IPTp &Malaria in Pregnancy Bill Brieger | 15 Nov 2016
Joint efforts, a key to success for the Malaria in Pregnancy Program in Luanda, Angola
A poster entitled “Joint efforts, a key to success for the Malaria in Pregnancy Program in Luanda, Angola” was presented by Jhony Juarez, Adolfo Sampaio, William R. Brieger, and Domingos F. Gueve from Jhpiego’s Angola Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 Angola, in response to WHO’s 2012 updated guidance on Intermittent Preventive Treatment in pregnancy (IPTp), revised its national malaria protocol to better address the fact that 25% of maternal mortality is caused by the disease. The new protocol was a collaborative effort of a national technical working group assisting the National Malaria Control Program (NMCP) including the National Reproductive Health Program, the national AIDS Institute, WHO, UNICEF, UNFPA and implementing partners of the U.S. Presidents Malaria Initiative (PMI).
Angola, in response to WHO’s 2012 updated guidance on Intermittent Preventive Treatment in pregnancy (IPTp), revised its national malaria protocol to better address the fact that 25% of maternal mortality is caused by the disease. The new protocol was a collaborative effort of a national technical working group assisting the National Malaria Control Program (NMCP) including the National Reproductive Health Program, the national AIDS Institute, WHO, UNICEF, UNFPA and implementing partners of the U.S. Presidents Malaria Initiative (PMI).
The updated Prevention and Treatment Manual for Malaria in Pregnancy, based on the revised protocol, was approved in 2014, and efforts continued with reviewing and updating training modules, job aids and monitoring tools that would reflect the additional doses of IPTp. The Ministry of Health, with support from partners, then disseminated these materials in the provinces and municipalities where they worked. USAID’s ForçaSaúde program, with support from PMI, worked with the Provincial Health Directorate of Luanda to build capacity of 297 health professionals to implement the new guidance in 78 health facilities of four municipalities, Belas, Cazenga, Cacuaco and Viana, with a combined population of 4.3 million.
 Comparing the IPTp data from the four municipalities between 2014 and 2015, one can see that the new guidance has started to take effect. In both years approximately 70,000 pregnant women received the first dose or around 60% of women registering for antenatal care (ANC). For the new third dose there was an increase of 85% (from 12,490 women to 23,046), and receipt of the fourth dose rose by 164% (3,345 to 8,839).
Comparing the IPTp data from the four municipalities between 2014 and 2015, one can see that the new guidance has started to take effect. In both years approximately 70,000 pregnant women received the first dose or around 60% of women registering for antenatal care (ANC). For the new third dose there was an increase of 85% (from 12,490 women to 23,046), and receipt of the fourth dose rose by 164% (3,345 to 8,839).
Two major challenges remain: increasing ANC registration and addressing missed opportunities to provide ANC doses for those who do attend including ensuring regular supplies of sulfadoxine-pyrimethamine for IPTp. Future progress requires continued inter-departmental collaboration among NMCP, Reproductive Health and the AIDs Institute, on-the-job training, enhanced statistical capacity, and supervision.
Diagnosis &HIV &Integration Bill Brieger | 25 Jul 2015
AIDS and Malaria: The Challenge of Co-Infection Persists
While the International AIDS Society is holding its 2015 meeting in Vancouver, it is important to remember that individual infectious diseases do not exist in isolation, but in combination make life worse for infected people. The co-infective culprit with HIV/AIDS that usually received the most attention is Tuberculosis, but malaria is not without its dangers. Herein we highlight a few recent studies and publications on the interactions between HIV and malaria.
Just because today malaria is primarily a tropical disease, it does not mean that people living with AIDS (PLHIV) in other parts of the world are not at risk. Schrumpf and colleagues point out that people living with HIV frequently travel to the tropics and thus may be at risk of infection by one of the species of malaria parasite. PLHIV are not unlike other travelers who do not always adhere with travel recommendations for using bednets and taking appropriate prophylaxis, but the consequence of non-adherence may be more severe.
In areas endemic for both malaria and HIV the effects of co-infection continue to be studied. In western Kenya Rutto and co-workers report that, “HIV-1 status was not found to have effect on malaria infection, but the mean malaria parasite density was significantly higher in HIV-1 positive than the HIV-1 negative population.” So do malaria prevention and treatment interventions mitigate any of these problems?
Kenya Rutto and co-workers report that, “HIV-1 status was not found to have effect on malaria infection, but the mean malaria parasite density was significantly higher in HIV-1 positive than the HIV-1 negative population.” So do malaria prevention and treatment interventions mitigate any of these problems?
Co-infection is not the only shared problem of these two diseases in areas where both are endemic. Yeatman et al. reported that, “In malaria-endemic contexts, where acute HIV symptoms are commonly mistaken for malaria, early diagnostic HIV testing and counseling should be integrated into health care settings where people commonly seek treatment for malaria.”
Mozambique has updated its guidelines for managing anemia among HIV-infected persons. The updated “guidelines for management of HIV-associated anemia prompts clinicians to consider opportunistic conditions, adverse drug reactions, and untreated immunosuppression in addition to iron deficiency, intestinal helminthes, and malaria.” Brentlinger and colleagues concluded that the guidelines are valuable in helping clinicians address anemia through a variety of interventions.
In areas where anti-retroviral treatment may be delayed, use of long lasting insecticide treated nets (LLINs) might help. Again in Kenya, Verguet and fellow researchers conducted a cost analysis and concluded that, “Provision of LLIN and water filters could be a cost-saving and practical method to defer time to ART eligibility in the context of highly resource-constrained environments experiencing donor fatigue for HIV/AIDS programs.”
Introduction of universal cotrimoxazole prophylaxis for all HIV positive patients in Uganda is seen to have a positive effect on reducing malaria infections among HIV positive patients. Rubaihayo and research partners found this effect as well as reported on several other studies with similar results.
One key overall lessons from these studies is the need to have integrated services for prevention, detection and management of both malaria and HIV. National health programs as well as global donors should make integrated service delivery a priority.
Health Systems &Human Resources &Integration &Malaria in Pregnancy Bill Brieger | 02 Nov 2014
Improved Malaria Services in Malawi: Jhpiego and USAID at ASTMH
 Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Malawi.
Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Malawi.
One of the panel presentations is “Improving Malaria Outcomes in Malawi: Focusing on Integration of Services at all Levels” presented by John Munthali, Senior Technical Advisor, Jhpiego/Malawi. John works with Support for Service Delivering Integration-Services (SSDI-S), a USAID bilateral program (2011-2016) with Partnerships in 15 Districts involving the Ministry of Health, Jhpiego, Save the Children International, Care Malawi and Plan International.
 SSDI-Services focuses on Malawi’s Essential Health Package (EHP) Focal Areas with particular emphasis on Maternal Health, Newborn and Child Health, Family Planning and Reproductive Health, HIV/AIDS and TB, Nutrition and Malaria. Aspects of the Malaria Component include Intermittent Preventive Treatment and Insecticide Treated Bed Nets
SSDI-Services focuses on Malawi’s Essential Health Package (EHP) Focal Areas with particular emphasis on Maternal Health, Newborn and Child Health, Family Planning and Reproductive Health, HIV/AIDS and TB, Nutrition and Malaria. Aspects of the Malaria Component include Intermittent Preventive Treatment and Insecticide Treated Bed Nets
SSDI-S is based on Promotion of the continuum of care from household to hospital. Health Facility Approaches address Improved Technical Capacity of Health Workers, Functional Health Facility, and Data-informed Decision Making. Community Approaches involve Improved Technical Capacity of CHWs, Functional Village Clinics, and Community Mobilization. Integration is a major concern such that there are no missed opportunities of EHP services at all levels.
Positive Trends since have been seen since Inception. Malaria in Pregnancy interventions supported the National Malaria Control program to review the Malaria in Pregnancy guidelines and training manuals to adopt the new WHO policy recommendations. 74 Trainers were trained in all 15 districts. MNCH services were established in selected districts. 344 HSAs were trained. 70 community-based Core Groups oriented on MNCH. SSDI supported ongoing MNCH activities through review meetings and distribution of reporting forms.
 As a result of these integrated high impact interventions there has been a remarkable increase in the uptake of IPTp 2 (16% in June 2012 to 64% in Sept. 2013) by pregnant women in the SSDI-services focus districts. Central to this increase is the integration of services at the facility level where malaria has been highly integrated into maternal, newborn and child health. The project has also seen IPTp 1 uptake maintained at above 91% in all the 15 districts
As a result of these integrated high impact interventions there has been a remarkable increase in the uptake of IPTp 2 (16% in June 2012 to 64% in Sept. 2013) by pregnant women in the SSDI-services focus districts. Central to this increase is the integration of services at the facility level where malaria has been highly integrated into maternal, newborn and child health. The project has also seen IPTp 1 uptake maintained at above 91% in all the 15 districts
Malaria Care capacity building has resulted in improved iCCM services delivered by Health Surveillance Assistants (HSAs) at village clinics. iCCM is serving as the foundation for community-based treatment of malaria by HSAs while at facility level IMCI provides an integrated approach to manage childhood illnesses including malaria.
In conclusion, it is feasible to integrate MNCH programs at all levels using SBCC and Systems Strengthening. Having an integrated project looking at the whole spectrum of health services (system strengthening, service delivery and behavior change) can help improve programming & service delivery.
Community &Integration &Treatment Bill Brieger | 11 Oct 2014
Is community case management sustainable in Mozambique? A qualitative policy analysis
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
 Below is an abstract by Baltazar Chilundo, Julie Cliff, Alda Mariano, Daniela Rodrigues, and Asha George of the University Eduardo Mondlane, Mozambique and the Johns Hopkins School of Public Health on the sustainability of community case management, building on longstanding community health worker programs. They stress the importance of community commitment, an often missing factor when CHW and CCM programs are organized by national agencies.
Below is an abstract by Baltazar Chilundo, Julie Cliff, Alda Mariano, Daniela Rodrigues, and Asha George of the University Eduardo Mondlane, Mozambique and the Johns Hopkins School of Public Health on the sustainability of community case management, building on longstanding community health worker programs. They stress the importance of community commitment, an often missing factor when CHW and CCM programs are organized by national agencies.
“In Mozambique, community case management (CCM) of diarrhoea, malaria and pneumonia is embedded in the national community health worker (CHW) programme. Since 1978 this programme functioned fitfully and was relaunched in 2010, with a target to train and retrain over 6000 CHWs.
 “Considering the checkered history of the CHW program, sustainability lies at the heart of concerns related to the design and implementation of CCM in CHW programs at scale in Mozambique and in people centred health systems more broadly.
“Considering the checkered history of the CHW program, sustainability lies at the heart of concerns related to the design and implementation of CCM in CHW programs at scale in Mozambique and in people centred health systems more broadly.
“Using qualitative retrospective case study methodology, we reviewed 54 national documents and interviewed 21 key national informants for a policy analysis of CCM in Mozambique. The data were analysed thematically according to a sustainability framework and validated though a national debriefing workshop.
“The sustainability of CCM was facilitated by embedding it in the national CHW programme, which was relaunched after wide consultation within government and with supportive donors and non-governmental organizations (NGOs).
“Although communities were not widely consulted, they were eager for CHWs to provide curative services. The new CHW program aimed to improve CHW retention, by paying them a salary and giving priority to females. However, salary costs come from partners and in practice most CHWs are male.
“The poor capacity of the health system to adequately supervise CHWs and guarantee drug supplies for CCM, the dependence on external partners for funding, and on NGOs for implementation and the lack of mobilization of communities and top policy makers remain critical concerns.
“Embedding CCM in the national CHW programme favoured sustainability, however this made CCM susceptible to the same factors that undermine sustainability of the CHW programme. Moving forward, these policy concerns need to be addressed to ensure a national CHW program, responsive to community needs, supportive of CHW themselves and owned by national governments.”
Health Systems &HIV &Integration Bill Brieger | 20 Jul 2014
Malaria at AIDS2014
Malaria and HIV/AIDS interact on several fronts from the biological, clinical, pharmacological to the service delivery levels. The ongoing 20th International AIDS Conference in Melbourne, Australia (July 20-25, 2014) provides an opportunity to discuss some of these issues. Abstracts that are available as of 20th July are mentioned below and deal largely with integrated health service delivery issues. Details can be found at http://www.aids2014.org/. Also keep up to date on twitter at https://twitter.com/AIDS_conference, and on Facebook at https://www.facebook.com/InternationalAIDSConference.
 1. Increasing HIV testing and counseling (HTC) uptake through integration of services at community and facility level (TUPE358 – Poster Exhibition). E. Aloyo Nyamugisa, B. Otucu, J.P. Otuba, L. Were, J. Komagum, F. Ocom, C. Musumali (USAID/NU-HITES Project, Plan International – Uganda, Gulu, Uganda).
1. Increasing HIV testing and counseling (HTC) uptake through integration of services at community and facility level (TUPE358 – Poster Exhibition). E. Aloyo Nyamugisa, B. Otucu, J.P. Otuba, L. Were, J. Komagum, F. Ocom, C. Musumali (USAID/NU-HITES Project, Plan International – Uganda, Gulu, Uganda).
HTC integration at community outreaches and facility service points increases service uptake by individuals, families and couples that come to access the different services that are offered concurrently such as immunization, family planning, cervical cancer screening, circumcision, Tuberculosis, malaria, nutrition screening services and other medical care.
2. Asymptomatic Malaria and HIV/AIDS co-morbidity in sickle cell disease (SCD) among children at Mulago Hospital, Kampala, Uganda (TUPE074 – Poster Exhibition). B.K. Kasule, G. Tumwine, (Hope for the Disabled Uganda, Kampala, Uganda, Watoto Child Care Ministries, Medical Department, Kampala, Uganda, Makerere University, College of Veterinary Medicine, Animal Resources & Bio-security, Kampala, Uganda).
The prevalence of HIV/AIDS and asymptomatic malaria in children attending SCD clinic were quite high with the former exceeding the national prevalence supporting the view than Ugandan children with SCD die before five years. Children were significantly stunted and underdeveloped which could have made them prone to increased clinic visits. National health programmes should focus on the health needs of children with SCD by integrating HIV/AIDS care, nutritional therapy, and malaria control programmes.
3. Technical support (TS) needs of countries for preparation of funding requests under the Global Fund’s new funding model (NFM) (THPE427 – Poster Exhibition). A. Nitzsche-Bell, B. Hersh (UNAIDS, Geneva, Switzerland).
The results of this survey suggest that there is very high demand GF funding in 2014 and a concomitant high demand for TS to assist in the preparation of funding requests. TS priority needs span across different technical, programmatic and management areas. Increased availability of funding for TS and enhanced partner coordination through the Country Dialogue process are needed to ensure that countries have access to timely, demand-driven, and high-quality TS to maximize mobilization of GF resources under the NFM.
4. Optimizing the efficiency of integrated service delivery systems within the existing scaled-up community health strategy in Kenya: pathfinder/USAID/APHIAplus Nairobi-Coast program experience (THPE351 – Poster Exhibition). V. Achieng Ouma, D.M. Mwakangalu, P. Eerens, J. Mwitari, E. Mokaya, J. Aungo Bwo’nderi, S. Naketo Konah (Pathfinder International, Nairobi, Kenya, Pathfinder International, Service Delivery, Mombasa, Kenya, Ministry of Health, Division of Community Health Strategy, Nairobi, Kenya, Pathfinder International, Research and Metrics/Strategic Information Hub, Nairobi, Kenya, University of Portsmouth, Geography, Portsmouth, United Kingdom).
APHIAplus (a USAID sponsored health program in Kenya) supports the implementation of integrated government strategies that center around HIV, AIDS, and tuberculosis prevention, treatment, and care; integrated reproductive health and family planning services; and integrated malaria prevention and maternal and newborn health services. Lessons learned include the finding that integrated outreach holds potential to meet clients’ needs in an efficient, effective manner. For example, during a single contact with a service provider, a mother obtains immunization services and growth monitoring for her infant, counseling and testing for HIV, counseling on family planning, cervical cancer screening, and treatment of minor ailments. Results indicate better integration of HIV prevention, care, and treatment within complementary efforts that address key drivers of mortality and morbidity. Success in integration was fostered by a stronger focus on outcomes throughout the APHIAplus implementation cycle.
5. Long term outcomes of HIV-infected Malawian infants started on antiretroviral therapy while hospitalized (THPE070 – Poster Exhibition). A. Bhalakia, M. Bvumbwe, G.A. Preidis, P.N. Kazembe, N. Esteban-Cruciani, M.C. Hosseinipour, E.D. Mccollum (Albert Einstein College of Medicine and Children’s Hospital at Montefiore, Pediatrics, Bronx, United States, Baylor College of Medicine Abbott-Fund Children’s Clinical Centre of Excellence, Lilongwe, Malawi, Baylor College of Medicine, Pediatrics, Houston, United States, University of North Carolina Project, Lilongwe, Malawi, Johns Hopkins School of Medicine, Pediatrics, Division of Pulmonology, Baltimore, United States).
![]() One-year retention rates of HIV-infected infants diagnosed and started on ART in the hospital setting are comparable to outpatient ART initiations in other Sub-Saharan countries. Further studies are needed to determine if inpatient diagnosis and ART initiation can provide additional benefit to this population, a subset of patients with otherwise extremely high mortality rates. Of the 16 children who died, median time from ART initiation to death was 2.7 months. Causes of death include pneumonia, diarrhea, fever, anemia, malnutrition, malaria and tuberculosis.
One-year retention rates of HIV-infected infants diagnosed and started on ART in the hospital setting are comparable to outpatient ART initiations in other Sub-Saharan countries. Further studies are needed to determine if inpatient diagnosis and ART initiation can provide additional benefit to this population, a subset of patients with otherwise extremely high mortality rates. Of the 16 children who died, median time from ART initiation to death was 2.7 months. Causes of death include pneumonia, diarrhea, fever, anemia, malnutrition, malaria and tuberculosis.
6. Killing three birds with one stone: integrated community based approach for increasing access to AIDS, TB and Malaria services in Oyo and Osun States of Nigeria (MOPE435 – Poster Exhibition). O. Oladapo, E. Olashore, K. Onawola, M. Ijidale. (PLAN Health Advocacy and Development Foundation, Programs, Ibadan, Nigeria, Civil Society for the Eradication of Tuberculosis in Nigeria, Programs, Ibadan, Nigeria, Community and Child Health Initiative (CCHI), Programs, Ibadan, Nigeria, Community Health Focus (CHeF), Programs, Ibadan, Nigeria).
Community Systems Strengthening (CSS) is a tested and successful strategy for providing integrated AIDS, TB and Malaria (ATM) services in resource-limited settings. 20 selected community based organizations (CBOs) working on at least one of AIDS, TB or Malaria were trained by PLAN Foundation on basics of ATM-related project management including monitoring and evaluation; demand generation through active referrals; and community outreaches. Empowering CBOs is an effective and low-cost strategy for increasing demand for ATM services in resource-limited settings. Integrating referral for ATM services increases effectiveness of and public confidence in primary healthcare services at the grassroots.
7. (Upcoming on 21st July) The health impact of a program to integrate household water treatment, hand washing promotion, insecticide-treated bed nets, and pediatric play activities into pediatric HIV care in Mombasa, Kenya (MOAE0104 – Oral Abstract Session). N. Sugar, K. Schilling, S. Sivapalasingam, A. Ahmed, D. Ngui, R. Quick. (Project Sunshine, New York, United States, U.S. Centers for Disease Control and Prevention, Division of Foodborne, Waterborne, and Environmental Diseases, National Center for Emerging and Zoonotic Infections, CDC, Atlanta, United States, New York University, New York, United States, Bomu Hospital, Mombasa, Kenya).