Health Systems &Malaria in Pregnancy Bill Brieger | 28 Jul 2014 11:38 am
Attending Antenatal Care Does Not Guarantee Antimalaria Services
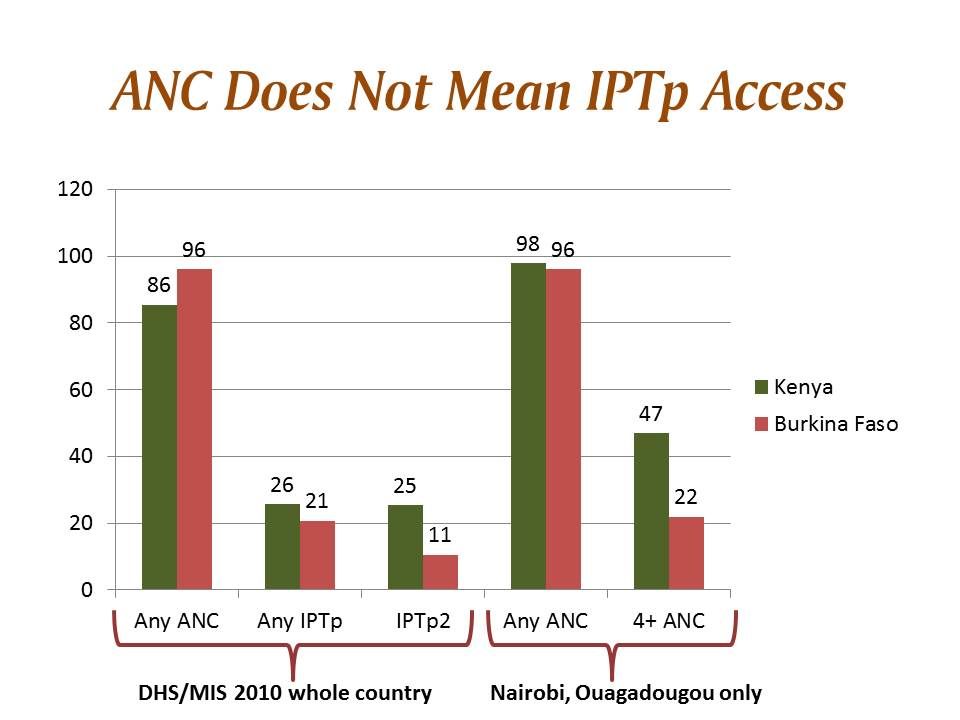
A new article by Clementine Rossier and colleagues compares access to maternal health services in Ouagadougou, Burkina Faso and Nairobi Kenya. In both settings a very large proportion of pregnant women registered for antenatal care (ANC). Twice the proportion of Nairobi women (47%) attended up to four times compared to those in Ouadougou (22%). In both settings, the likelihood of attending four ANC visits increased with educational level of the women.
 Although the article does not discuss services received at ANC, we can consider the implications for malaria in pregnancy (MIP) control since ANC is a major platform for MIP service delivery. Here the demographic and health survey (DHS) and its malaria indicator survey (MIS) component are of help. Both countries had a national survey in 2010 (their most recent).
Although the article does not discuss services received at ANC, we can consider the implications for malaria in pregnancy (MIP) control since ANC is a major platform for MIP service delivery. Here the demographic and health survey (DHS) and its malaria indicator survey (MIS) component are of help. Both countries had a national survey in 2010 (their most recent).
Interestingly in 2010 Burkina Faso overall had better ANC registration (05%) than Kenya (86%). In neither country was intermittent preventive treatment in pregnancy (IPTp) coverage good. 25.7% of pregnant women in Kenya received one dose of sulfadoxine-pyrimethamine for IPTp, while 20.8% did so in Burkina Faso. IPTp2 coverage in Kenya was similar at 25.4%, but in Burkina Faso it dropped to 10.6%
 The important lesson here is that even with good ANC registration, women have no guarantee of receiving life saving malaria prevention services. If registration was lower we might suspect issues of local beliefs and other community barriers, but the situation in both countries points to health systems failures like inadequate drug supplies and health worker lapses.
The important lesson here is that even with good ANC registration, women have no guarantee of receiving life saving malaria prevention services. If registration was lower we might suspect issues of local beliefs and other community barriers, but the situation in both countries points to health systems failures like inadequate drug supplies and health worker lapses.
The service delivery situation in both countries has changed dramatically since 2010. Kenya has refined its malaria map and is focusing IPTp on areas of stable and high transmission. Burkina Faso has received greater influx of financial support from the Global Fund and the US Agency for International Development. Hopefully the 2014 DHS/MIS studies currently in progress in both countries will paint a better picture. Of course, unless health systems issues are being addressed, funding alone will not solve the malaria service gaps.