Case Management &CHW &IPTp &ITNs Bill Brieger | 14 Apr 2018
Community Health Volunteers Contribute to Improved Malaria Prevention and Management in Kribi, Cameroon
Kodjo Morgah, Eric Tchinda, and Naibei Mbaïbardoum of Jhpiego (a Johns Hopkins University Affiliate) in Cameroon are presenting a poster at the Multilateral Initiative for Malaria Conference in Dakar this week. Their findings, seen below, show how community health volunteers can contribute to improving the quality of malaria control services in Chad and Cameroon.

CHV Lilian Kubeh preparing to administer a rapid diagnostic test. Photo by Karen Kasmauski.
Project objectives focused overall on contributing to the reduction of malaria-related morbidity and mortality in Cameroon and Chad. It also aimed to strengthen community-based interventions through the use of community health volunteers (CHVs) to manage simple cases of malaria and conduct awareness-raising activities. The geographic scope of the project was Kribi District in the south of Cameroon. Thirty-two health facilities are supported by Jhpiego. Kribi District has an estimated population of 134,876.
Reports from the National Malaria Control Program show that malaria is the leading cause of morbidity in Cameroon—an estimated 1,500,000 cases occur each year. In 2016, it was the leading reason for medical consultations (23.6% of all medical consultations) and hospitalizations (46% of all hospitalizations). Among children under 5 years of age, malaria accounted for 41% of all medical consultations and 55% of all hospitalizations. Malaria is also a leading cause of mortality. In 2016, Cameroon had 2,639 deaths caused by malaria—12% of all deaths across all age groups and 28% of all deaths among children under 5 years of age were attributed to malaria.
 Project intervention strategies target the four levels of the health system. The CHV intervention was mobilized to support the strategy at the community level as seen in the attached diagram. In 2012 and 2014, 38 CHVs were selected by the community and received training to support areas in the district more than 10 km from a health center. (Note: 10 km was the measurement tool used to determine the geographic scope of each CHV for this project.) An initial donation of medications, data collection tools, and small equipment was made available to CHVs using funding from ExxonMobil Foundation. An evaluation of the training intervention was conducted by an external consultant in April 2016.
Project intervention strategies target the four levels of the health system. The CHV intervention was mobilized to support the strategy at the community level as seen in the attached diagram. In 2012 and 2014, 38 CHVs were selected by the community and received training to support areas in the district more than 10 km from a health center. (Note: 10 km was the measurement tool used to determine the geographic scope of each CHV for this project.) An initial donation of medications, data collection tools, and small equipment was made available to CHVs using funding from ExxonMobil Foundation. An evaluation of the training intervention was conducted by an external consultant in April 2016.

CHV Daniel Ze conducting an individual educational session on IPTp. Photo by Karen Kasmauski.
CHVs conduct outreach activities in their communities—via home visits and community education sessions—to provide health education on malaria transmission and prevention, use of long-lasting insecticidal nets, the importance of intermittent preventive treatment in pregnancy (IPTp), and the importance of promptly seeking medical care for suspected cases of malaria. CHVs also support national health campaigns and health promotion events, including World Malaria Day. In Cameroon, where CHVs are also able to test and treat patients, they administer rapid diagnostic tests (RDTs) and treat cases of uncomplicated malaria.
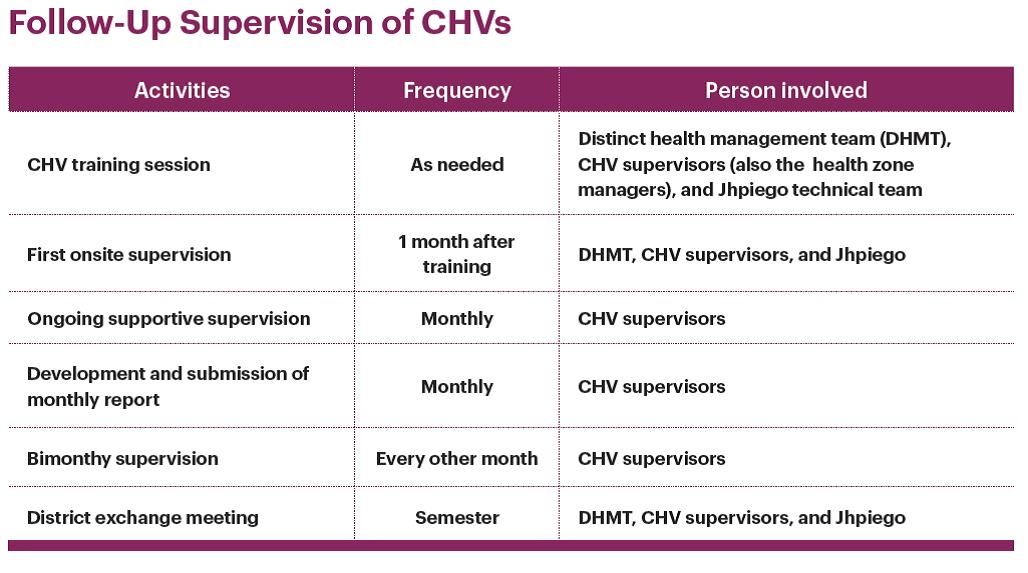 Motivation of CHVs included ongoing training and technical updates, regular replenishment of materials, CHVs are recognized and respected community leaders, provision of per diem and transport costs, and continued advocacy targeting district officials to provide CHV stipends to ensure sustainability. Attached are details of the supervisory activities that provided continual technical support to the CHVs to ensure that they retain knowledge and skills to carry out their activities and track their data.
Motivation of CHVs included ongoing training and technical updates, regular replenishment of materials, CHVs are recognized and respected community leaders, provision of per diem and transport costs, and continued advocacy targeting district officials to provide CHV stipends to ensure sustainability. Attached are details of the supervisory activities that provided continual technical support to the CHVs to ensure that they retain knowledge and skills to carry out their activities and track their data.
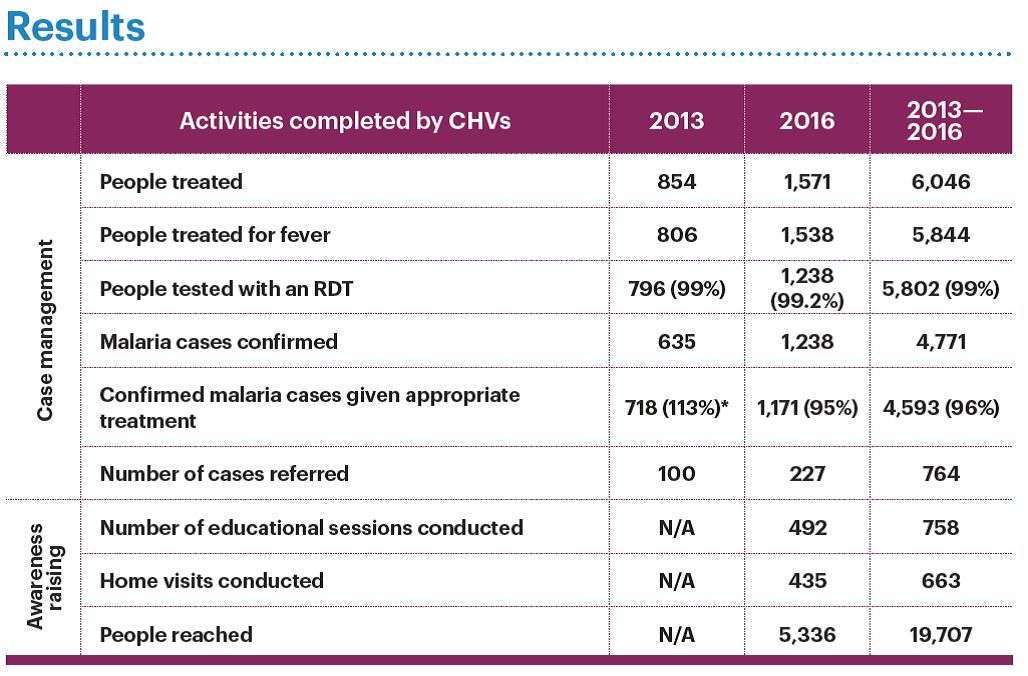 Between 2013 and 2016 CHVs in these communities were able to reach nearly 20,000 people with a variety of malaria services as seen in the attached table. The project paid close attention to data quality, which was reviewed with the CHVs on a regular basis, resulting in improved data quality. CHVs improved the accessibility of malaria prevention and care services for communities living in remote areas. Results from April 2016 external evaluation show these results. Knowledge of malaria prevention is significantly higher in households that did not receive CHV support (p = 0.001). Use of long-lasting insecticide-treated nets is higher in households that benefitted from CHV support (88%) than in households that did not benefit from CHV support (73%) (p = 0.023). There was an increase in the delivery of IPTp2, from 60% in 2012 to 70% in 2016.
Between 2013 and 2016 CHVs in these communities were able to reach nearly 20,000 people with a variety of malaria services as seen in the attached table. The project paid close attention to data quality, which was reviewed with the CHVs on a regular basis, resulting in improved data quality. CHVs improved the accessibility of malaria prevention and care services for communities living in remote areas. Results from April 2016 external evaluation show these results. Knowledge of malaria prevention is significantly higher in households that did not receive CHV support (p = 0.001). Use of long-lasting insecticide-treated nets is higher in households that benefitted from CHV support (88%) than in households that did not benefit from CHV support (73%) (p = 0.023). There was an increase in the delivery of IPTp2, from 60% in 2012 to 70% in 2016.
In conclusion CHVs have increased their communities’ access to health centers through referrals, health education on malaria prevention, IPTp, and treatment for simple and severe cases of malaria. Regular supervision of CHVs by their supervisors (the health zone managers) is essential to maintaining and strengthening CHV performance and motivation. Continuing advocacy efforts with local authorities is necessary to ensure that CHV activities are sustainable. The project team aims to establish a mechanism to improve documentation of its activities to better measure the impact on indicators at the community, facility, and district levels, and provide evidence for advocacy to sustain these efforts.
Community &Primary Health Care Bill Brieger | 13 Apr 2018
Malaria and Primary Health Care: 40 Years after Alma Ata
The Concept of Primary Health Care (PHC) was formalized in 1978 when The World Health Organization and UNICEF convened a major conference in the then Alma Ata in Kazakhstan. The resulting Alma Ata Declaration resulted in advocacy for Health for All, which had evolved into Universal Health Coverage. The Declaration outlined important principles such as community participation in health care planning and delivery, promotion of scientifically sound and acceptable health interventions, the use of community-based health workers (CHWs), and addressing the common endemic health problems in each community. One of those endemic problems common to a majority of communities in Africa is malaria. Now in 2018, 40 years after the Alma Ata Declaration we explore how malaria has progressed within the context of PHC.
 The Roll Back Malaria Partnership (RBM) began in 1998, 20 years after Alma Ata. When RBM convened a meeting of African Heads of State in 2000 the resulting Abuja Declaration set targets for major malaria interventions of 80% coverage by 2010. The Abuja Declaration reflected principles of Alma Ata when it called on all member states to undertake health systems reforms which will:
The Roll Back Malaria Partnership (RBM) began in 1998, 20 years after Alma Ata. When RBM convened a meeting of African Heads of State in 2000 the resulting Abuja Declaration set targets for major malaria interventions of 80% coverage by 2010. The Abuja Declaration reflected principles of Alma Ata when it called on all member states to undertake health systems reforms which will:
- Promote community participation in joint ownership and control of Roll Back Malaria actions to enhance their sustainability.
- Make diagnosis and treatment of malaria available as far peripherally as possible including home treatment.
- Make appropriate treatment available and accessible to the poorest groups in the community.
By 2011 reality intervened. WHO reported that “In the 10 years that has passed since the Abuja Declaration, there has been progress towards increasing the availability of financial resources for health at least in terms of dollar values. However, there has not been appreciable progress in terms of the commitments the Africa Union governments make to health, or in terms of the proportion of GNI the rich countries devote to Overseas Development Assistance.” Since that time funding from international and bilateral donors has leveled, such that there is even greater need for malaria endemic countries to step forward and guarantee access to malaria prevention and treatment services are available through PHC at the grassroots. Such access needs to move beyond removing barriers to making malaria interventions attractive to the community.

Community Health Workers in Nigeria are trained to provide malaria community case management
Christopher and colleagues looked to the community and examined how response to malaria and other childhood illnesses were faring 30 years since Alma Ata. After they reviewed seven studies of community health workers they concluded that “CHWs in national programmes achieved large mortality reductions of 63% and 36% respectively, when insecticide-treated nets and anti-malarial chemoprophylaxis were delivered, in addition to curative interventions.” (They found little evidence of the effectiveness of these community interventions on pneumonia and diarrhoea.) The challenge they saw was the ability of countries to move beyond successful studies to scale up and sustain community malaria control interventions to the national level and thereby reap the full promises and benefits of PHC.
Others continue to advocate for a community role in achieving malaria goals through PHC. Malaria Consortium has looked at the position of malaria control within the context of Community Based PHC (CBPHC) and the use of CHWs as a means for revisiting Health for All.

Community donates a house in Western Region Ghana to serve as CHPS Compound where malaria services are provided to the community
Ghana’s community-based health planning and services (CHPS) program aims to make primary care accessible at the grass roots. CHPS compounds are small clinics in space usually donated by the community, staffed by community health officers who oversee community based agents (CBAs) and other community volunteers who treat and prevent malaria through integrated community case management. Countries have also build on the community directed intervention approach pioneered by the African Program for Onchocerciasis Control to ensure malaria interventions are delivered through community community planning and action.
Controlling and eventually eliminating malaria will certainly go a long way toward helping achieve Health for All. On this 40th Anniversary year of Alma Ata it is time to ensure that all malaria endemic countries and malaria donors revisit the basic philosophy of community action and participation and ensure that these principals guide us to accessible and sustainable malaria programming by the community “Through their Full Participation.”
![]() (This posting has been extracted from a full article appearing in the April 2018 Issue of Africa Health. Also please join the discussion about Alma Ata at 40 on the forum created by colleagues at the Johns Hopkins Bloomberg School of Public Health.)
(This posting has been extracted from a full article appearing in the April 2018 Issue of Africa Health. Also please join the discussion about Alma Ata at 40 on the forum created by colleagues at the Johns Hopkins Bloomberg School of Public Health.)
Case Management &CHW &Elimination &Malaria in Pregnancy Bill Brieger | 11 Apr 2018
Multilateral Initiative for Malaria (MIM) – Jhpiego Presents in Dakar
 The 7th Pan African Malaria Conference holds from 15-20 April 2017, Dakar, Senegal. The conference celebrates 20 years since the initial establishment of the Multilateral Initiative on Malaria (MIM) by the Tropical Disease Research Program and partners.
The 7th Pan African Malaria Conference holds from 15-20 April 2017, Dakar, Senegal. The conference celebrates 20 years since the initial establishment of the Multilateral Initiative on Malaria (MIM) by the Tropical Disease Research Program and partners.
During the conference next week, staff from Jhpiego malaria projects in Burkina Faso, Liberia, Nepal, Madagascar and Cameroon will share oral and poster presentations to highlight their work. Below is a list along with the location numbers.
- Application d’un Audit de la Qualité des données (DQA) du paludisme dans le District Sanitaire de Kribi, Cameroun, SS-13 Oral
- Contribution des Agent de Santé Communautaire (ASC) à l’amélioration de la prévention et la prise en charge du paludisme dans le district de Kribi, Cameroun, B-40 Poster
- MOH’s effort in developing and implementing Quality Assurance plan (QAP) for Global Fund-supported antimalarial drugs: A case study of Nepal in the context of malaria elimination, C-107 Poster
- Community-Based Health Workers in Burkina Faso: Are they ready to take on a larger role to prevent malaria in pregnancy? D-115 Poster

- Contribution of Community-Based Health Workers (CBHWs) to Improving Prevention of Malaria in Pregnancy in Burkina Faso: Review of health worker perceptions from the baseline study D-118 Poster
- Malaria in Pregnancy: The Experience of MCSP in Liberia, D-140 Poster
- Improved Malaria Case Management of Under-Five Children: The Experience of MCSP-Restoration of Health Liberia project D-141 Poster
- Experiences and perceptions of care seeking for febrile illness among caregivers, pregnant women and health providers in eight districts of Madagascar D-142 Poster

 Abstracts will be shared here on the day of each presentation for those unable to attend MIM. Also check Jhpiego at Exhibit Booth 148.
Abstracts will be shared here on the day of each presentation for those unable to attend MIM. Also check Jhpiego at Exhibit Booth 148.
Treatment &Universal Coverage &Women Bill Brieger | 07 Apr 2018
Health Insurance, Malaria and Universal Coverage
World Health Day 2018 is promoting universal health coverage. National Health Insurance Schemes (NHIS) are seen as a way to foster universal health coverage by improving access to basic, life-saving care. In malaria-endemic countries, NHIS hopefully play a role in reducing malaria mortality. For example in Nepal, malaria was among the chronic and communicable illnesses that showed increased catastrophic health expenditure over time leading to impoverishment. Health insurance was seen as a way to counteract this problem.
Although health insurance coverage in Tanzania was quite low, “a higher proportion of women with health insurance had a proper timing of 1st ANC attendance compared to their counterparts.” This enables them to access malaria prevention services and interventions.
 Ghana has been operating a NHIS since 2003. Overall national coverage has been estimated at around 40%, with a greater proportion of women covered than men. The 2014 Demographic and Health and 2016 Malaria Indicator Surveys (DHS, MIS) show that around 60% of women of reproductive age have NHIS coverage. How does this translate into malaria service coverage?
Ghana has been operating a NHIS since 2003. Overall national coverage has been estimated at around 40%, with a greater proportion of women covered than men. The 2014 Demographic and Health and 2016 Malaria Indicator Surveys (DHS, MIS) show that around 60% of women of reproductive age have NHIS coverage. How does this translate into malaria service coverage?
 In Ghana a decrease in malaria deaths was seen against a backdrop of increased admissions owing to free access to hospitalization through the NHIS, but hospital admission is not an option for all. Community case management is aimed at increasing access to and coverage of timely management of malaria and other child illnesses, but such services may not be covered by a NHIS. Since iCCM is effective in reaching children, Ghana is questioning how community based health workers can be brought into the health insurance arena.
In Ghana a decrease in malaria deaths was seen against a backdrop of increased admissions owing to free access to hospitalization through the NHIS, but hospital admission is not an option for all. Community case management is aimed at increasing access to and coverage of timely management of malaria and other child illnesses, but such services may not be covered by a NHIS. Since iCCM is effective in reaching children, Ghana is questioning how community based health workers can be brought into the health insurance arena.
Rwanda started its community based health insurance scheme in 2003 also and by 2013 had achieved 74% coverage. In Rwanda community malaria action teams (CMATs) were initiated in mid-2014 as platforms to deliver malaria preventive messages at village level. Among other benefits of the CMATs, an increase in community-based health insurance membership occurred,

Mutuelle (community health insurance) kiosk outside a clinic in Burkina Faso
which was also considered as a predictor of prompt and adequate care. Another study in Rwanda showed that head of household having health insurance (among other factors) was significantly associated with prompt and adequate care for presumed malaria illness.
NHIS have their own challenges in terms of affordability, community understanding of payment of premiums and availability of points of care that accept insurance or are accredited. And not all endemic countries have achieved even the modest successes of NHIS in Ghana and Rwanda. Thus health insurance offers hope for expanding universal coverage of malaria services, but health systems and community understanding and participation need to be improved for this to happen.
CHW &Diagnosis &Elimination &Epidemiology Bill Brieger | 01 Apr 2018
Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia
Global Health Day 2018 sponsored by the Johns Hopkins University Center for Global Health featured a poster presentation by several colleagues on Improving the efficacy of reactive screen-and-treat for malaria elimination in southern Zambia. Fiona Bhondoekhan, William Moss, Timothy Shields, Douglas Norris, Kelly Searle, Jennifer Stevenson, Harry Hamapumba, Mukuma Lubinda and Japhet Matoba (Southern Africa International Centers of Excellence in Malaria Research, the JHU Bloomberg School of Public Health, and the Macha Research Trust, Zambia) share their findings below.
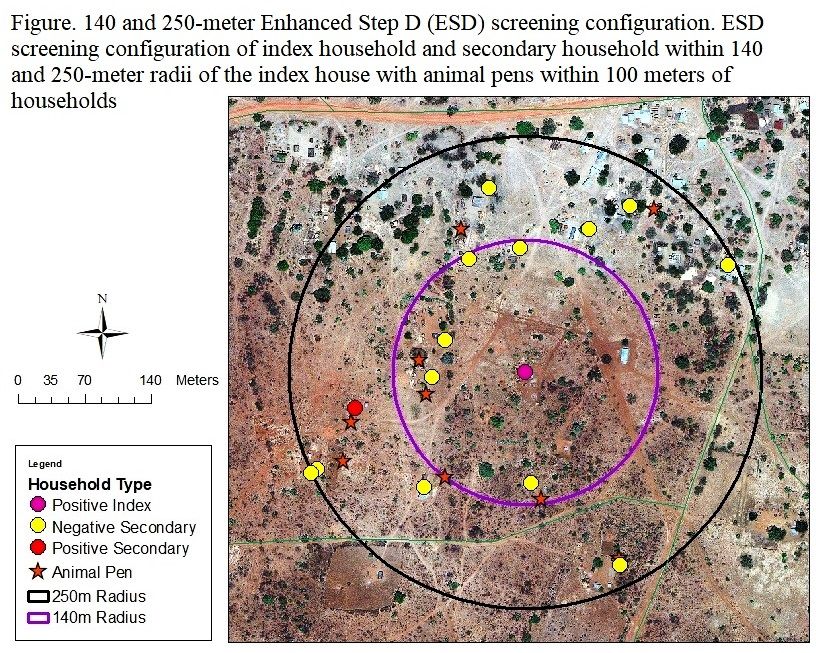 Background: Malaria screen-and-treat (called Step D in Zambia) is a reactive case detection strategy in which cases detected at a health center trigger community health workers (CHWs) to screen for secondary malaria cases within a 140-meter radius of the index case household using PfHRP2 rapid diagnostic tests (RDTs). Few studies evaluated whether an evidence-based strategy using environmental features that characterize the immediate surroundings of a household, can improve the efficiency of secondary case identification.
Background: Malaria screen-and-treat (called Step D in Zambia) is a reactive case detection strategy in which cases detected at a health center trigger community health workers (CHWs) to screen for secondary malaria cases within a 140-meter radius of the index case household using PfHRP2 rapid diagnostic tests (RDTs). Few studies evaluated whether an evidence-based strategy using environmental features that characterize the immediate surroundings of a household, can improve the efficiency of secondary case identification.
Objective: This study utilized the Step D and extended the screening radius to 250-meters (termed Enhanced Step D or ESD) to assess which local environmental variables can guide CHWs to identify secondary cases more efficiently. As Zambia works toward eliminating malaria, more refined and targeted case detection strategies are required to find the untreated malaria cases that could serve as potentially asymptomatic sources of infection. This study can help guide and plan reactive case detection strategies in Zambia that allow community health workers/field teams to employ an evidence-based strategy to find malaria-positive secondary households situated near index case houses more efficiently.
 Methods: Demographic information, malaria diagnosis, bed-net use and ownership, cooking energy source, and household floor material were obtained from surveys. Households were stratified into malaria positive and negative secondary households using RDT and qPCR results. ArcGIS was used to generate the following local environmental variables: screening radius (140 vs. 250-meters), number of animal pens within 100-meters, distance to nearest animal pen, distance and elevation difference between index and secondary houses, as well as the following large scale environmental variables: distance to main road and nearest stream category. Generalized estimating equations (GEE) estimated the cross-sectional effect for the difference in odds of a positive vs. negative secondary household for each predictor. For the secondary analysis GEE with the same model specifications was used to estimate the cross-sectional difference in odds of a positive vs. negative household for each environmental predictor. Model fit was evaluated with the Hosmer-Lemeshow goodness of fit test and significance was evaluated as a p-value of 0.05. Statistical analyses were carried out using STATA 14.2.
Methods: Demographic information, malaria diagnosis, bed-net use and ownership, cooking energy source, and household floor material were obtained from surveys. Households were stratified into malaria positive and negative secondary households using RDT and qPCR results. ArcGIS was used to generate the following local environmental variables: screening radius (140 vs. 250-meters), number of animal pens within 100-meters, distance to nearest animal pen, distance and elevation difference between index and secondary houses, as well as the following large scale environmental variables: distance to main road and nearest stream category. Generalized estimating equations (GEE) estimated the cross-sectional effect for the difference in odds of a positive vs. negative secondary household for each predictor. For the secondary analysis GEE with the same model specifications was used to estimate the cross-sectional difference in odds of a positive vs. negative household for each environmental predictor. Model fit was evaluated with the Hosmer-Lemeshow goodness of fit test and significance was evaluated as a p-value of 0.05. Statistical analyses were carried out using STATA 14.2.
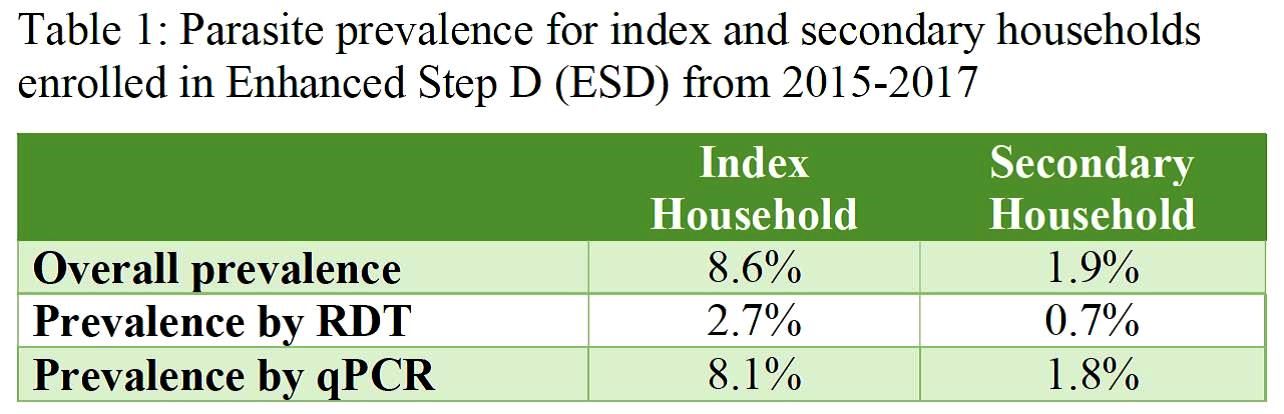
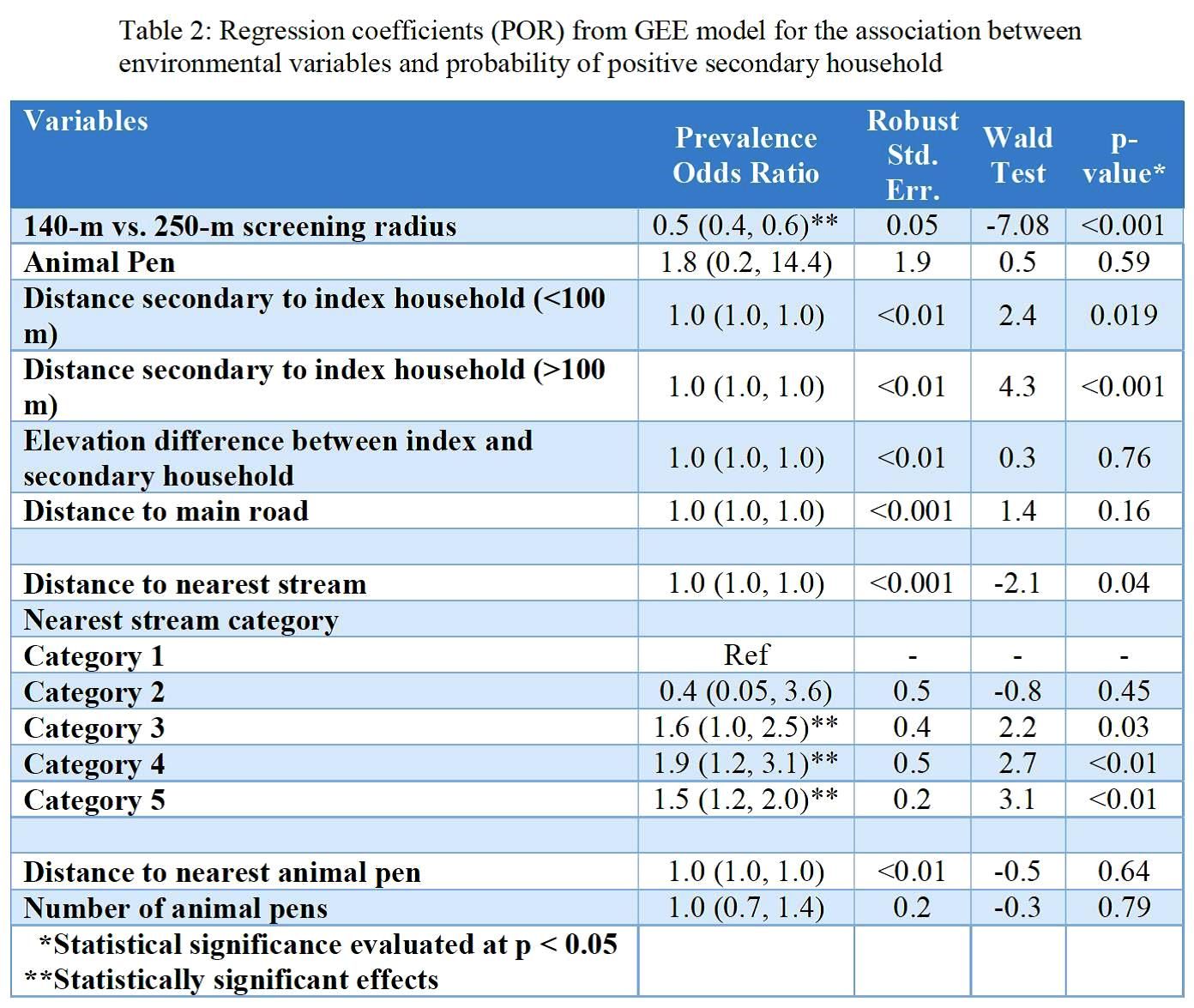 Results: Screening within the index households yielded an overall parasite prevalence of 8.6%, which was higher by qPCR (8.1%) than RDT (2.7%) as seen in Table 1. Secondary households had an overall parasite prevalence of 1.9% with similar differences by test used. Key results from regression analysis seen in Table 2 include a difference in prevalence according to screening radius as well as by proximity to the nearest stream. Secondary analysis produced similar results but showed statistically significant higher odds for households where animal pens were present.
Results: Screening within the index households yielded an overall parasite prevalence of 8.6%, which was higher by qPCR (8.1%) than RDT (2.7%) as seen in Table 1. Secondary households had an overall parasite prevalence of 1.9% with similar differences by test used. Key results from regression analysis seen in Table 2 include a difference in prevalence according to screening radius as well as by proximity to the nearest stream. Secondary analysis produced similar results but showed statistically significant higher odds for households where animal pens were present.
Conclusion: Screening for secondary households within low-transmission setting in Zambia could be optimized by using both local-scale indicators such as the presence of animal pens and large-scale indicators such as streams as environmental guiding tools.
Acknowledgements: This research was supported in part the Bloomberg Philanthropies and the Johns Hopkins Malaria Research Institute, and the NIH-sponsored Southern and Central Africa ICEMR 2U19AI089680.
