Ebola Bill Brieger | 27 Oct 2015
Documenting the Response to the Ebola Epidemic in Liberia through the Perspective of the Local Press
 Join Kwame Sakyi and William R. Brieger of the he Johns Hopkins University at ASTMH Annual Meeting Afternoon Scientific Session #87 on Ebola on Tuesday at 1.45 pm to learn more about how the Liberian Press portrayed Ebola as seen in the Abstract below.
Join Kwame Sakyi and William R. Brieger of the he Johns Hopkins University at ASTMH Annual Meeting Afternoon Scientific Session #87 on Ebola on Tuesday at 1.45 pm to learn more about how the Liberian Press portrayed Ebola as seen in the Abstract below.
Mass media play an important role in documenting national responses to crises like Ebola. Reviewing media documentation helps a country better prepare for current and future public health challenges. Ebola articles first appeared in the Liberian press in March 2014. Our objectives were to determine the frequency of newspaper accounts and the major issues covered.
We conducted content analysis of Ebola coverage in three Liberian newspapers from March through December 2014. We reviewed electronic publications of three main newspapers by searching for the term “Ebola”.
 Data collected for each article included date of publication, and topic. Data were compiled in Microsoft Excel. After reading the first 50 articles, we inductively generated codes to capture the news content and compiled these into a codebook. The codebook was constantly refined as additional articles were read. Codes were organized into major themes.
Data collected for each article included date of publication, and topic. Data were compiled in Microsoft Excel. After reading the first 50 articles, we inductively generated codes to capture the news content and compiled these into a codebook. The codebook was constantly refined as additional articles were read. Codes were organized into major themes.
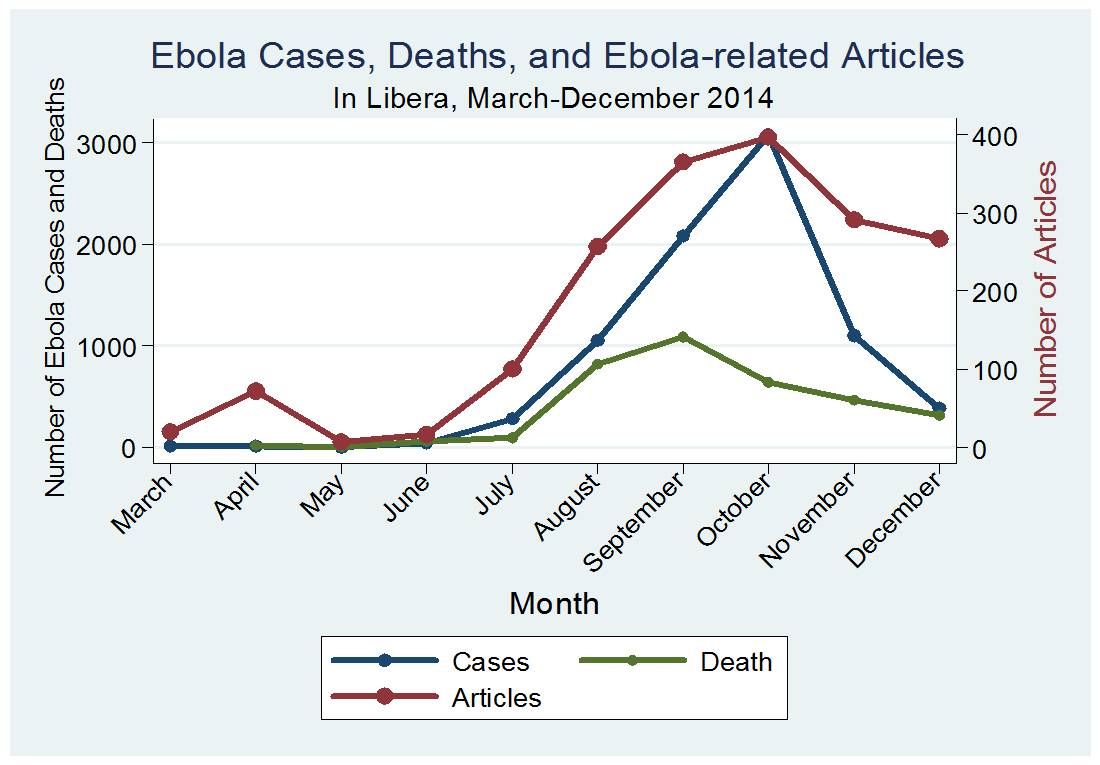
A total of 1,793 articles were published across the 3 newspapers over the 10-month period. The frequency of publications on Ebola ranged from 27 in March 2014, but increased to 95 April. Coverage dropped to only 15 in June, but began to rise sharply in August (227), reaching its peak in October (345).
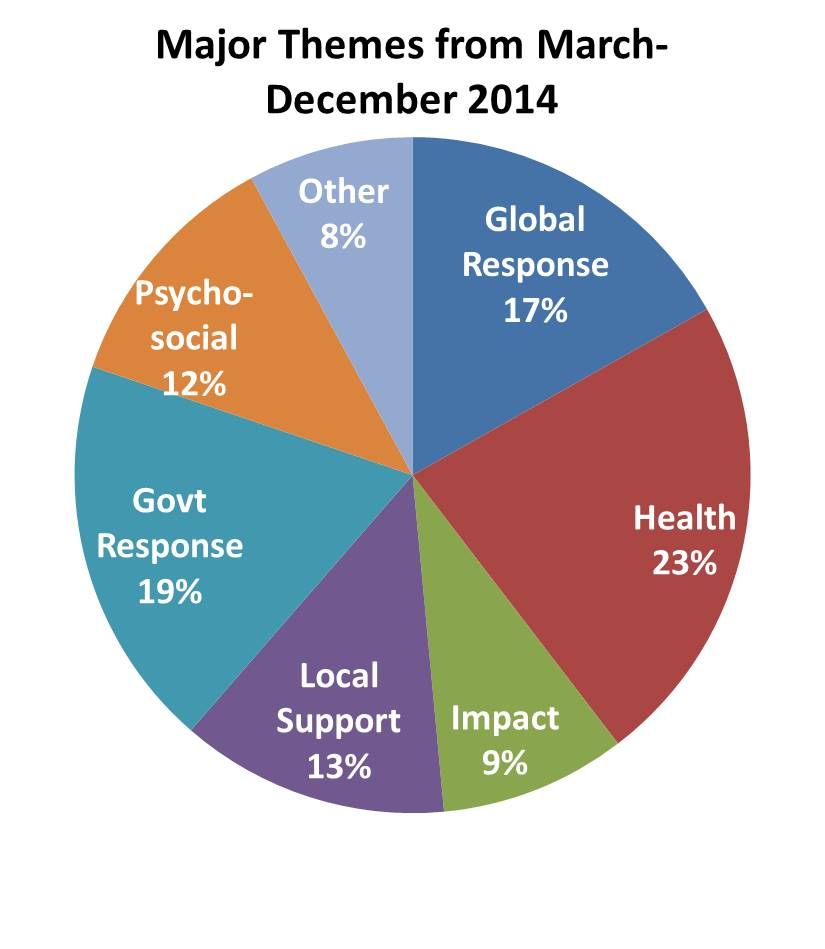 News reports frequency paralleled the incidence pattern of the disease. Major themes included the state of the epidemic, health care, psychosocial issues, international aid, political response, prevention, and local support. Overall political response to Ebola and the impact of Ebola on health workers received the most attention. In the early days common themes were border security and requests for aid.
News reports frequency paralleled the incidence pattern of the disease. Major themes included the state of the epidemic, health care, psychosocial issues, international aid, political response, prevention, and local support. Overall political response to Ebola and the impact of Ebola on health workers received the most attention. In the early days common themes were border security and requests for aid.
At the peak key themes were health worker problems and political responses. A review of the national press during a crisis like Ebola provides a valuable overview of the response of the different players ranging from health services and NGOs to international partners and government. It reflects political will and conflicts and can help a central operations team better coordinate resources and responses of partners.
Elimination &IPTp &ITNs Bill Brieger | 27 Oct 2015
Winning the fight against malaria in Huambo Province, Angola
Colleagues[1] from the Ministry of Health, Huambo, Angola and Jhpiego are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster LB-5246 and discuss the results as presented in the Abstract below.
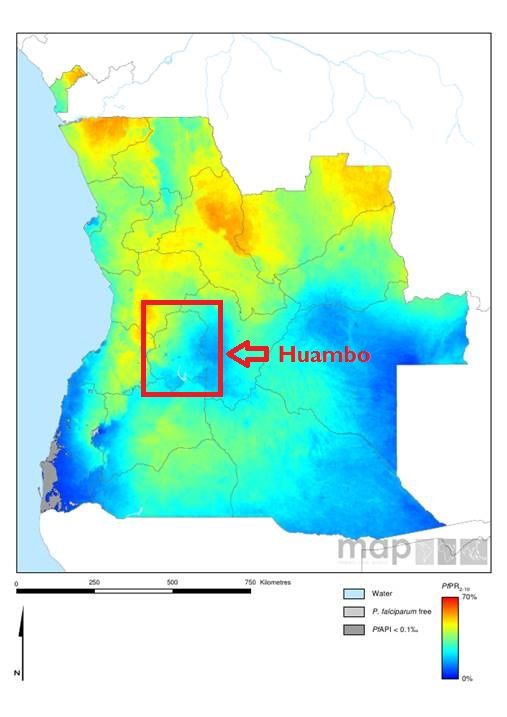 Huambo is on of Angola’s 18 provinces, with close to 2 million inhabitants. Traditionally malaria has accounted for a large portion of clinic consultations, hospitalizations, and child and maternal mortality. Angola has three epidemiological strata: hyper-endemic area (north), meso-endemic stable area (central area), where Huambo is located, and meso-endemic unstable area (south).
Huambo is on of Angola’s 18 provinces, with close to 2 million inhabitants. Traditionally malaria has accounted for a large portion of clinic consultations, hospitalizations, and child and maternal mortality. Angola has three epidemiological strata: hyper-endemic area (north), meso-endemic stable area (central area), where Huambo is located, and meso-endemic unstable area (south).
The main malaria vector is Anopheles gambiae (ss, melas and arabiensis) and Anopheles funestus. Parasitological studies show 85% of cases are P falciparum and 15% are P vivax.
The Huambo Provincial Health Directorate has been working with stakeholders including national and international NGOs, traditional leaders, churches, religious leaders, police, army and media to fight malaria. This collaboration is showing results.
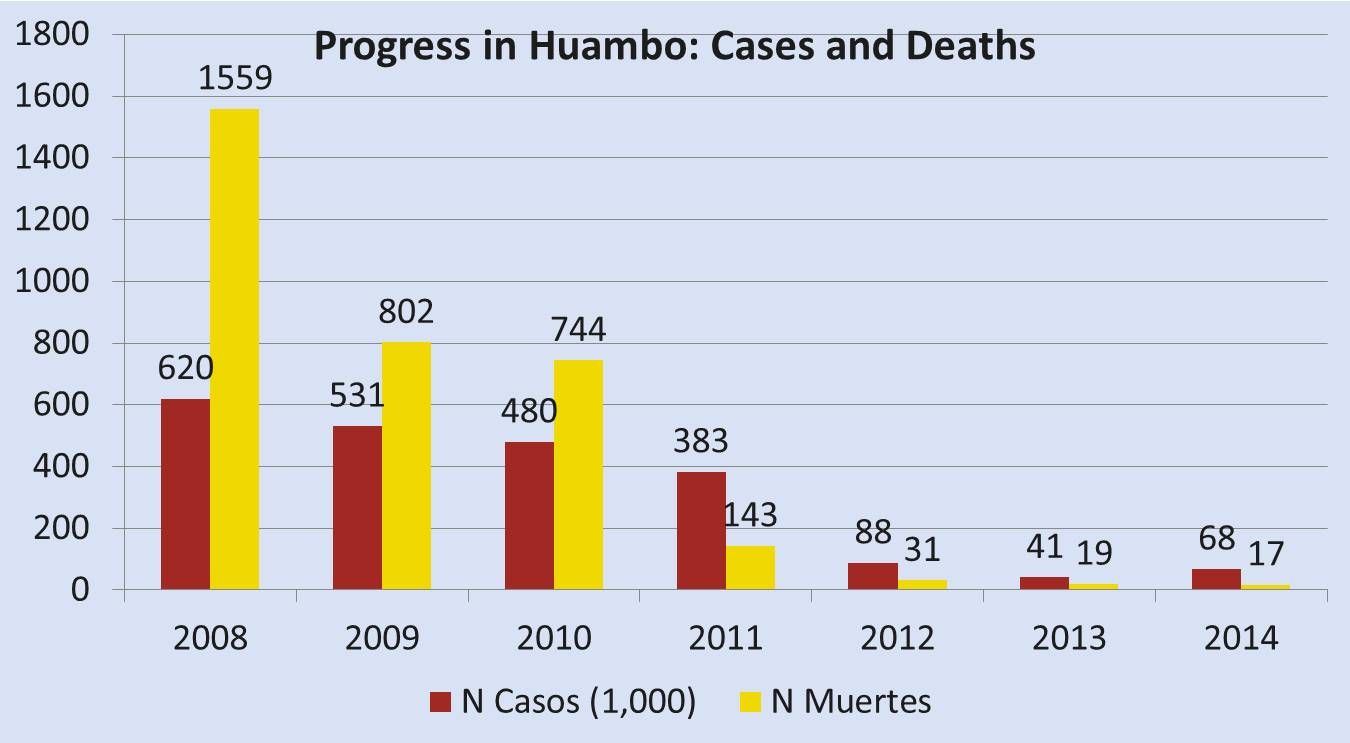 Cases have dropped steadily from 620,300 in 2008 to 68,547 in 2014. Likewise deaths have declined from 1,559 to 17 in the same period. During this period there has been an increase in training and supervision of health professionals to improve their malaria prevention, diagnosis and treatment skills.
Cases have dropped steadily from 620,300 in 2008 to 68,547 in 2014. Likewise deaths have declined from 1,559 to 17 in the same period. During this period there has been an increase in training and supervision of health professionals to improve their malaria prevention, diagnosis and treatment skills.
Rapid diagnostic tests have been deployed to all health units. Work with community organizations has resulted in health fairs (Uhayele Vimbo) in more remote locations. Over the most recent 5-year period the number of antenatal care clients receiving two doses of IPTp with SP has increased from 10,938 to 68,183 or from 30% to 54%.
Finally 330,000 ITNs were distributed between 2010 and 2014. The Province and its organizational and community partners are committed to sustaining these achievements in order to further reduce malaria morbidity and mortality.
[1] João Carlos F. Juliana, Jhony Juarez, Clementino Sacanombo, William R. Brieger
Advocacy &IPTp &Malaria in Pregnancy Bill Brieger | 26 Oct 2015
Health systems strengthening: Advocacy facilitates availability of sulfadoxine-pyrimethamine for prevention of malaria in pregnancy in Kenya
Colleagues[1] from Jhpiego’s Kenya office and the Ministry of Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster LB-5225 and discuss the results as presented in the Abstract below.
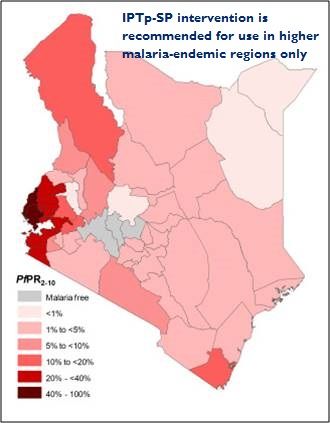 In malaria endemic areas, infection with malaria during pregnancy is often associated with poor pregnancy outcomes. Although effective intervention measures are available including use of sulfadoxine pyrimethamine (SP) for intermittent preventive treatment of malaria in pregnancy (IPTp) coverage rates have remained low.
In malaria endemic areas, infection with malaria during pregnancy is often associated with poor pregnancy outcomes. Although effective intervention measures are available including use of sulfadoxine pyrimethamine (SP) for intermittent preventive treatment of malaria in pregnancy (IPTp) coverage rates have remained low.
In Kenya, IPTp2 is at 38% in malaria endemic counties some of the key factors influencing IPTp uptake being SP stock-outs. The national government has been supplying SP but on devolution of health services to county governments it became the responsibility of the counties. There are many competing financial demands at county level and SP stock out is frequent.
 In February 2015 the national government disseminated a memo to county governments advising them to procure SP to avert the worsening SP stock out situation. After issuance of the memo, USAID’S flagship Maternal and Child Survival Program (MCSP) held discussions with the County Directors of Health (CDHs) and shared the quantification formula for SP requirement for the respective counties.
In February 2015 the national government disseminated a memo to county governments advising them to procure SP to avert the worsening SP stock out situation. After issuance of the memo, USAID’S flagship Maternal and Child Survival Program (MCSP) held discussions with the County Directors of Health (CDHs) and shared the quantification formula for SP requirement for the respective counties.
MCSP advocated for procurement of SP especially during the peak malaria transmission period May-August 2015. The CDHs on realizing the cost was not high made immediate arrangements for procurement of SP.
Bungoma County procured enough SP tablets to cover the peak malaria transmission season and distributed them to the health facilities. Results on analysed ANC data from facilities showed that the number of pregnant women accessing IPTp had reduced from 7,845 in October 2014 to 3,856 in February 2015.
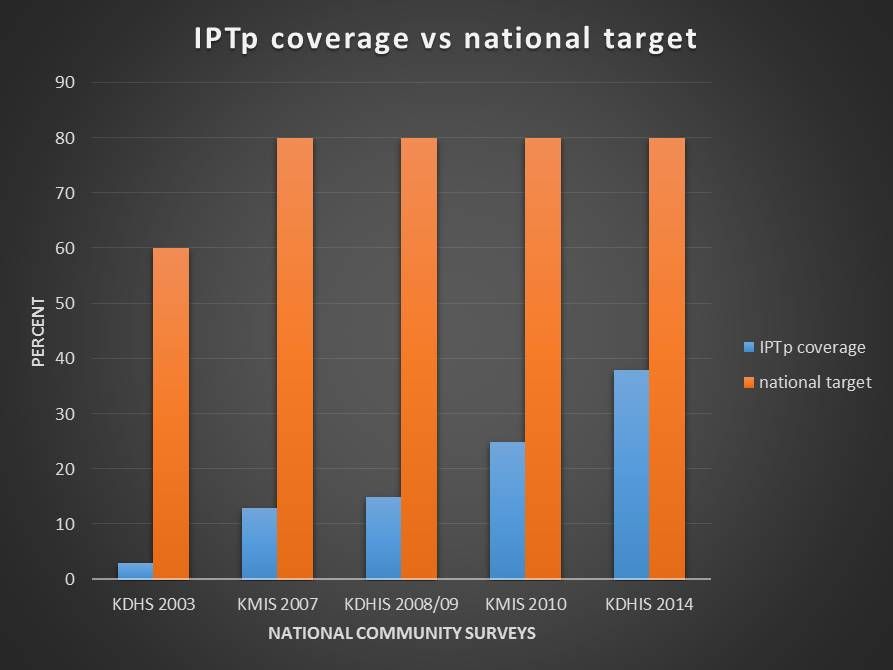 One month after procurement and distribution of SP, the number accessing SP increased from 3,856 to 6,769. To improve pregnancy outcomes in malaria endemic areas it is vital to reduce the effects of malaria during pregnancy. Use of IPTp-SP during pregnancy has been shown to improve pregnancy outcomes however, coverage rates of the intervention have remained below the national target due to several influencing factors like the SP stock-out situation experienced in Kenya.
One month after procurement and distribution of SP, the number accessing SP increased from 3,856 to 6,769. To improve pregnancy outcomes in malaria endemic areas it is vital to reduce the effects of malaria during pregnancy. Use of IPTp-SP during pregnancy has been shown to improve pregnancy outcomes however, coverage rates of the intervention have remained below the national target due to several influencing factors like the SP stock-out situation experienced in Kenya.
The use of advocacy with relevant authorities in Bungoma County leading to improvement in the SP stock out situation is considered a best practice in ensuring health commodity security and is being replicated in other malaria endemic counties.
[1] Augustine M. Ngindu, Gathari G. Ndirangu, Wekesa Kubasu, Isaac M. Malonza
Malaria in Pregnancy &Quality of Services Bill Brieger | 26 Oct 2015
Institutionalization of Quality of Care in Health Facilities Improves Management of Malaria in Pregnancy in Tanzania
Jasmine W. Chadewa and Rita Mutayoba of Jhpiego’s Dar es Salaam, Tanzania, office are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster 680 and discuss the results as presented in the Abstract below.
 Malaria in Pregnancy (MiP) is one of the contributors to maternal mortality in Tanzania which persists at a ratio of 410/100,000 live births. Tanzania implements WHO’s three-pronged approach to prevent MiP (use of insecticide treated bednets (ITNs), intermittent preventive treatment (IPTp) with sulfadoxine-pyrimethamine (SP) and prompt diagnosis and treatment).
Malaria in Pregnancy (MiP) is one of the contributors to maternal mortality in Tanzania which persists at a ratio of 410/100,000 live births. Tanzania implements WHO’s three-pronged approach to prevent MiP (use of insecticide treated bednets (ITNs), intermittent preventive treatment (IPTp) with sulfadoxine-pyrimethamine (SP) and prompt diagnosis and treatment).
Efforts are ongoing to improve IPTp and ITN coverage which is 33% and 75%, respectively. Jhpiego, in collaboration with the Ministry of Health and Social Welfare, worked in 251 health facilities to improve the quality of maternal and neonatal health by building the capacity of health care providers through training, supportive supervision, mentoring and coaching. A total of 7,181 providers and 400 tutors were trained on MiP prevention and treatment.
A quality of care study used the same methodology and sampling approach in 2010 and 2012, combining observations of women during antenatal care, inventory and record review as well as health worker knowledge. A team of MNH experts underwent clinical updates, training and orientation to the study tools.
 Data collection teams visited facilities, made observations and entered data into smart phones. The study was conducted in 12 regional hospitals and 38 lower level facilities in 12 regions including Zanzibar with a total of 391 and 366 ANC observations made in 2010 and 2012, respectively.
Data collection teams visited facilities, made observations and entered data into smart phones. The study was conducted in 12 regional hospitals and 38 lower level facilities in 12 regions including Zanzibar with a total of 391 and 366 ANC observations made in 2010 and 2012, respectively.
Between 2010 and 2012, the percentage of women receiving an ITN increased by 26% (p value = <0.0001). The change observed was due to a 33% increase in offering ITN vouchers at health centers and dispensaries. A slight improvement was seen in provision of IPTp(SP) from 62% in 2010 to 65% in 2012.
In Tanzania, application of the quality improvement approach contributed to improving MiP services. Moving forward, there is a need for the Ministry to continue strengthening ANC with effective monitoring and routine supervision to increase coverage of MiP prevention. Districts management teams and facilities need to ensure availability of SP and provide regular technical updates on the national service standards including counseling at ANC and birth preparedness.
Human Resources &IPTp &Training Bill Brieger | 26 Oct 2015
Improving provision of malaria services through provider training in Burkina Faso
Colleagues[1] from Jhpiego’s Burkina Faso Improving Malaria Care USAID-supported project and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster 969 and discuss the results as presented in the Abstract below.
 In 2013, malaria was the main reason for consultation (53.90%), hospitalization (63.20%) and death (49.60%) in health facilities; children under 5 and pregnant women are most affected. Recent revisions to the World Health Organization’s (WHO) guidance to maintain effective approaches to defeating malaria, include monthly dosing of intermittent preventive treatment for pregnant women (IPTp), starting from the 13th week of gestation.
In 2013, malaria was the main reason for consultation (53.90%), hospitalization (63.20%) and death (49.60%) in health facilities; children under 5 and pregnant women are most affected. Recent revisions to the World Health Organization’s (WHO) guidance to maintain effective approaches to defeating malaria, include monthly dosing of intermittent preventive treatment for pregnant women (IPTp), starting from the 13th week of gestation.
To align with the latest WHO guidance, the Burkina Faso Ministry of Health, with support from the USAID-funded Improving Malaria Care (IMC) project, revised national malaria guidelines in March 2014. 68 trainers from 9 health regions were trained on the revised national malaria guidelines.
From June to September 2014, 744 providers from 524 health facilities in 21 districts (33%) were trained on the prevention and management of malaria cases. To ensure updated guidance reaches all health workers, the training included a module on how to update colleagues in their respective facilities.
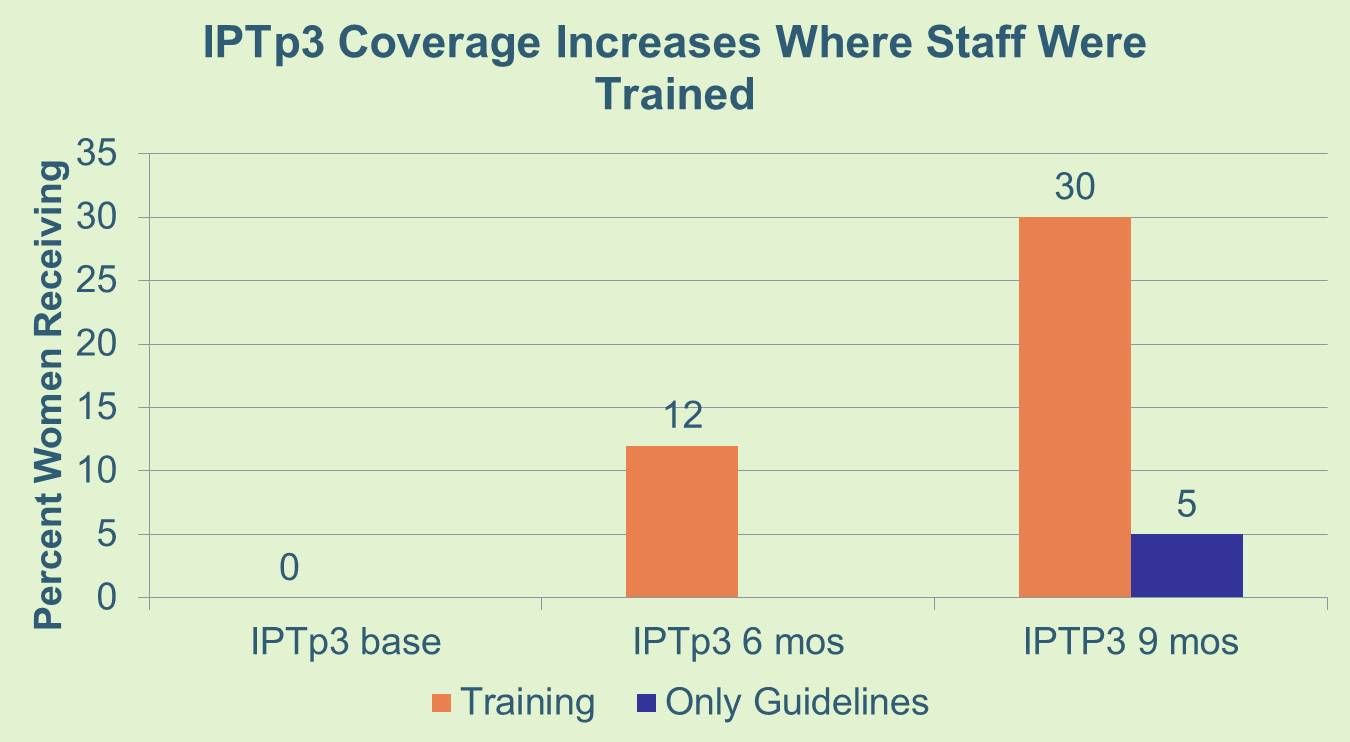 During supervision visits, most trained providers were using the new guidelines and pregnant women are increasingly receiving the third and higher doses of SP before delivery. In the first six months after the training sessions, pregnant women, who received the third dose of SP (IPTp3) increased from 0% to 12%. Three months later, that proportion rose to 30%. Comparatively, in the remaining 42 districts who received only the copies of the new guideline without training, IPTp3 was 5% nine months after receiving the guidelines.
During supervision visits, most trained providers were using the new guidelines and pregnant women are increasingly receiving the third and higher doses of SP before delivery. In the first six months after the training sessions, pregnant women, who received the third dose of SP (IPTp3) increased from 0% to 12%. Three months later, that proportion rose to 30%. Comparatively, in the remaining 42 districts who received only the copies of the new guideline without training, IPTp3 was 5% nine months after receiving the guidelines.
The training sessions contributed to improving the implementation of revised IPTp guidelines and uptake of IPTp 3 and higher better than distribution of the new guidelines alone. As a result the IMC project will scale-up the training in Year 2 to 600 more providers from 464 health facilities, and other partners have also agreed to support the National Malaria Control Program to reach remaining facilities. Challenges in increasing IPTp uptake include commodity distribution and inadequate engagement of private health facilities to update their practices and reporting of SP distribution.
[1] Ousman Badolo, Stanislas Nebie, Moumouni Bonkoungou, Mathurin Dodo, Thierry Ouedraogo, Rachel Waxman, William R. Brieger
Malaria in Pregnancy &Performance Bill Brieger | 26 Oct 2015
Health Systems Strengthening: Improving quality of services for prevention of malaria in pregnancy through the Standards-Based Management and Reward approach in Kenya
Colleagues[1] from the USAID-MCSP Project and Jhpiego (an affiliate of the Johns Hopkins Bloomberg School of public Health) are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster 385 and discuss the results as presented in the Abstract below
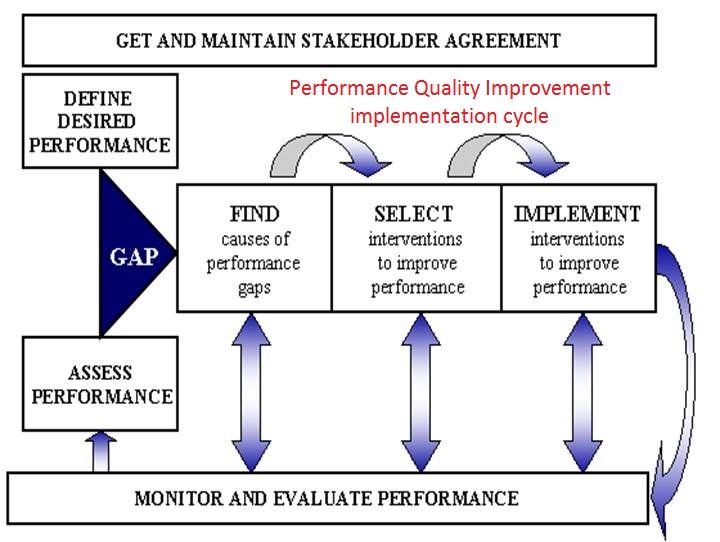 Performance quality improvement (PQI) is one of Jhpiego’s 9 health systems strengthening components in provision of health services towards improvement of maternal health including better pregnancy outcomes. The Standards-Based Management and Reward (SBM-R) approach has been used in improving as well as assessing the quality of services provided at health facilities.
Performance quality improvement (PQI) is one of Jhpiego’s 9 health systems strengthening components in provision of health services towards improvement of maternal health including better pregnancy outcomes. The Standards-Based Management and Reward (SBM-R) approach has been used in improving as well as assessing the quality of services provided at health facilities.
Kenya developed 15 malaria in pregnancy (MIP) SBM-R standards for use by service providers in provision of MIP services and is also used by supervisors to assess the quality of services provided at service delivery points. Facility incharges were trained on the 15 MIP SBM-R performance standards and they oriented service providers in their facilities on use of the performance standards.
 A baseline on SBM-R practices was done in all facilities before orientation in Kakamega east and Kakamega central subcounties and 1st assessment on practices done after three months of practice. A total of 30 health facility incharges from the two malaria endemic subcounties (Kakamega east 16 Kakamega central 14) were trained on the 15 MIP SBM-R performance standards.
A baseline on SBM-R practices was done in all facilities before orientation in Kakamega east and Kakamega central subcounties and 1st assessment on practices done after three months of practice. A total of 30 health facility incharges from the two malaria endemic subcounties (Kakamega east 16 Kakamega central 14) were trained on the 15 MIP SBM-R performance standards.
The facility incharges oriented 291 service providers (127 Kakamega east, 164 Kakamega central) on use of SBM-R performance standards in provision of MIP services in health facilities. Baseline assessment had an average score of 57% for Kakamega east and 58% for Kakamega central.
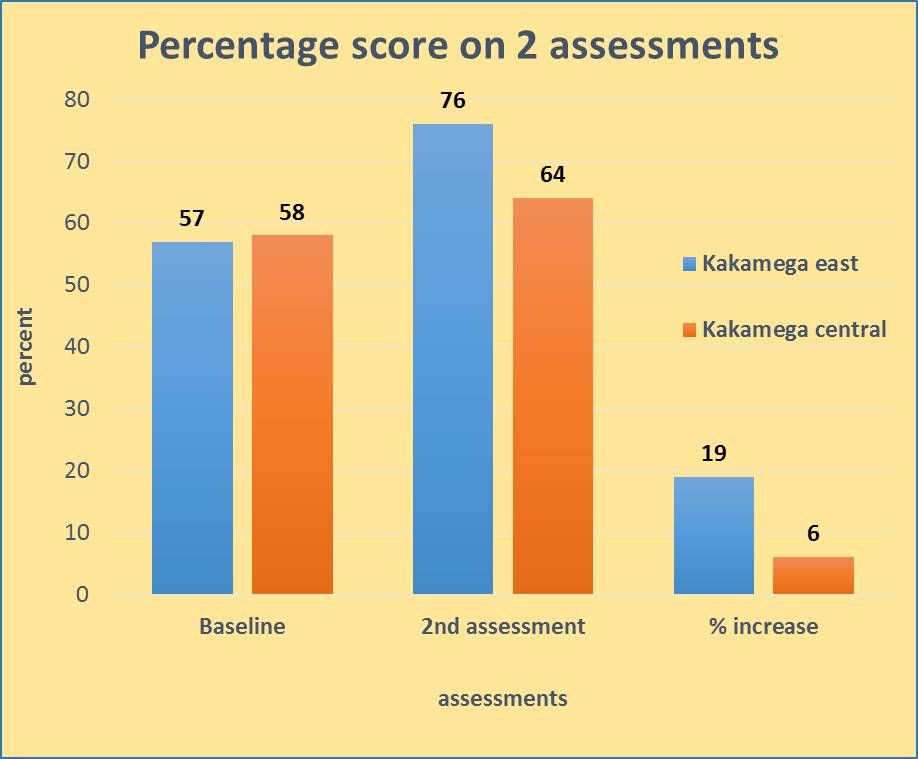 1st assessments were conducted after three months of practice and showed an average score of 76% for Kakamega east and 64% for Kakamega central giving an overall increase in score of 19% and 13% between baseline and 1st assessment for Kakamega east in Kakamega central respectively.
1st assessments were conducted after three months of practice and showed an average score of 76% for Kakamega east and 64% for Kakamega central giving an overall increase in score of 19% and 13% between baseline and 1st assessment for Kakamega east in Kakamega central respectively.
Use of MIP SBM-R performance standards ensures services provided at health facility level are in line with WHO recommendations and national guidelines. Establishment of PQI as a health systems strengthening component is feasible and is an approach that would make available quality MIP services at facility level. Provision of quality MIP services ensures protection of pregnant women against the effects of malaria in pregnancy.
[1] Augustine M. Ngindu, Gathari Ndirangu, Sanyu N. Kigondu, Isaac M. Malonza
Elimination &Epidemiology Bill Brieger | 26 Oct 2015
Readiness for Malaria Elimination: Using HMIS data to Map Malaria Test Positivity in Huambo Province, Angola
 Colleagues[1] from the Ministry of Health Angola, Jhpiego and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster LB-5094 and discuss the results as presented in the Abstract below.
Colleagues[1] from the Ministry of Health Angola, Jhpiego and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster LB-5094 and discuss the results as presented in the Abstract below.
Huambo Province in the south central highlands of Angola has a population of nearly 2 million, or 15% of the nation’s total. It is classified in the stable meso-endemic belt of the country, but is in the process of revising its malaria strategy to bring it closer to the pre-elimination phase on the pathway to malaria elimination. This means aiming to achieve 5% slide positivity rate for malaria parasites during the height of the transmission season (Novemb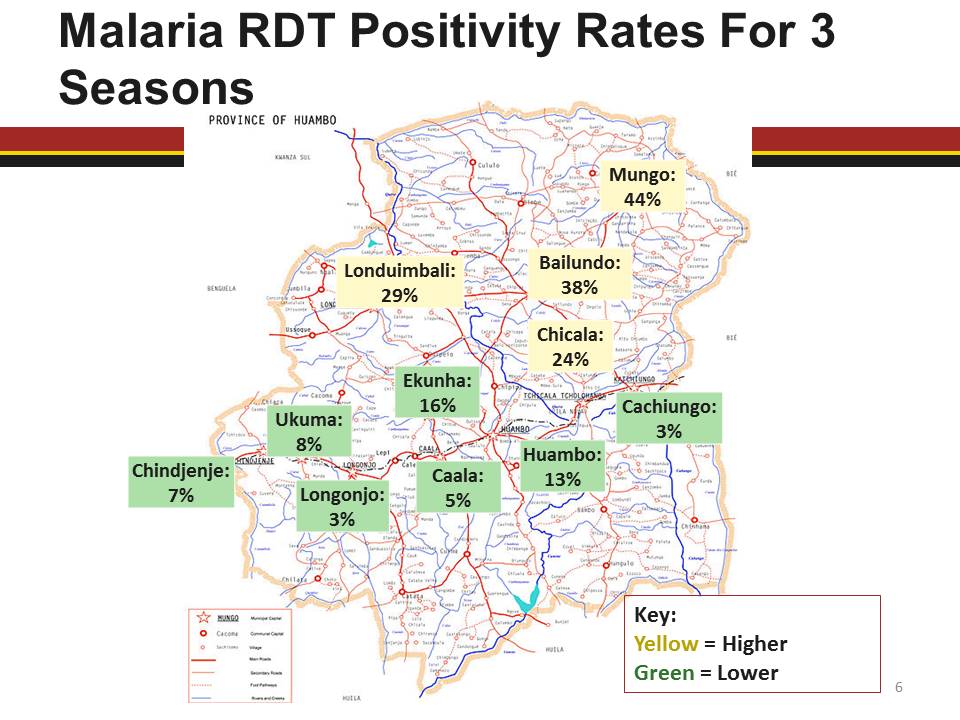 er to January).
er to January).
The health information system of the country reports information of positive and negative results of testing for suspected malaria cases from hospitals and clinics. The former use microscopy, while the latter rely on malaria rapid diagnostic tests (mRDTs). This information was analyzed for the past three high transmission periods and variations are reported herein among the 11 municipalities (districts) of the province.
The overall test positivity rates for all three seasons were 11% for microscopy and 25% for mRDTs among the 212,102 persons tested. The 4 municipalities in the northern part of the province ranged from 16-26% slide positivity and 24-44% mRDT positivity. The remaining municipalities in the south and central area ranged from 1-5% slide positivity and 3-16% mRDT positivity. Only one municipality achieved a positivity rate of <5% for both tests.
Moving forward, Huambo first intends to improve on the quality and coverage of malaria testing. The Ministry of Health will also focus on sustained control measures in the north, and begin more detailed mapping of malaria incidence in the central and southern municipalities to provide better targeting of interventions.
——-
[1] João Carlos F. Juliana, William R. Brieger, Jhony Juare3, Connie Lee, Clementino Sacanombo
Epidemiology &Malaria in Pregnancy Bill Brieger | 25 Oct 2015
Prevalence and Factors Associated with Malaria in Pregnancy in Rural Rwandan Health Facilities: A Cross-sectional Study
Colleagues[1] from the Rwanda Ministry of Health, Jhpiego and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster 315 and discuss the results as presented in the Abstract below.
Malaria in pregnancy (MIP) is a serious health risk for the pregnant woman and fetus and associated 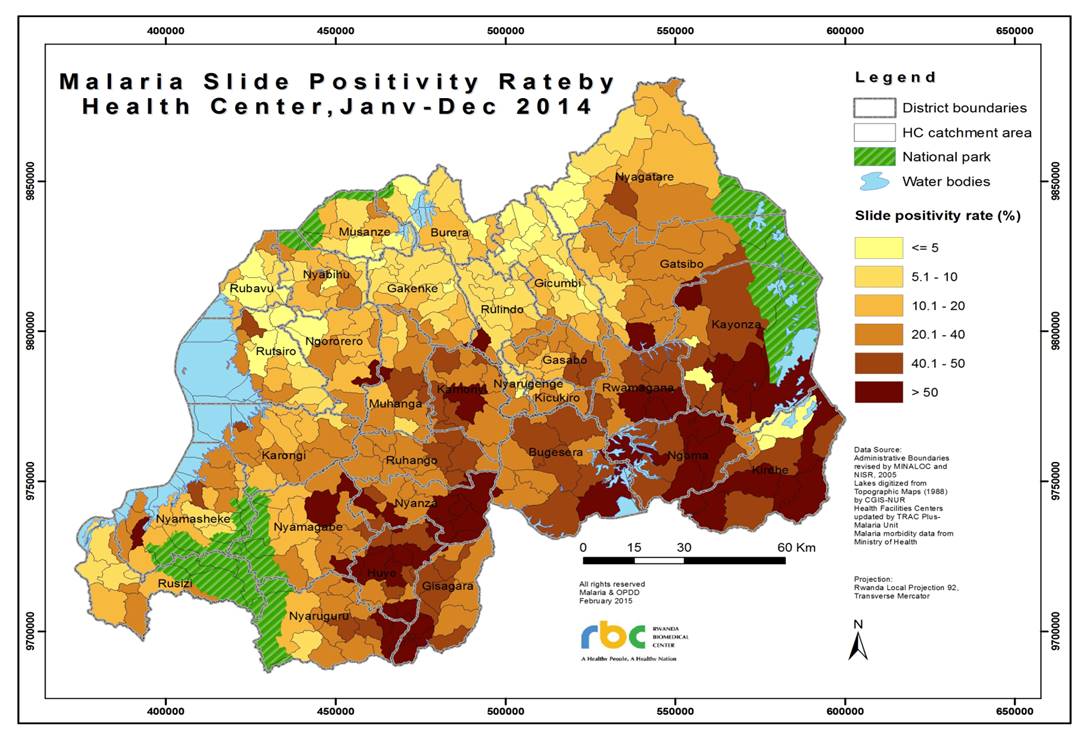 with mortality in the perinatal period. In Rwanda there has been no accurate national estimate of malaria prevalence among pregnant women. In 2011, a cross-sectional study of 6 districts in 3 malaria transmission zones (low, medium and high) in Rwanda was conducted to estimate the prevalence of peripheral parasitemia in pregnant women. Data were collected from consenting women presenting to antenatal clinics (ANC) for the first time in their current pregnancy including age, parity, gestation, ITN availability and use.
with mortality in the perinatal period. In Rwanda there has been no accurate national estimate of malaria prevalence among pregnant women. In 2011, a cross-sectional study of 6 districts in 3 malaria transmission zones (low, medium and high) in Rwanda was conducted to estimate the prevalence of peripheral parasitemia in pregnant women. Data were collected from consenting women presenting to antenatal clinics (ANC) for the first time in their current pregnancy including age, parity, gestation, ITN availability and use.
Blood was obtained for malaria testing using microscopy, rapid diagnosis tests and polymerase chain reaction (PCR). A total of 4,037 pregnant women were recruited with median age of 27 years, and 3,781 (93.7%) had usable PCR samples. The prevalence of MIP by PCR was 5.6%.
 Nearly 20% of women’s families did not have a net, and 8.7% of these tested positive compared to 4.9% of women whose family owned an ITN. For those who did not sleep under an ITN the previous night, 8.1% tested positive compared with 4.8% who slept under an ITN. Malaria prevalence by parity ranged from 5.5% (parity 0-1), to 5.4% (parity 2-3), and 6.5% (parity 4 or more). The two districts that bordered highly endemic countries had MIP prevalence rates of 10% and above. Those testing positive were treated according to national guidelines.
Nearly 20% of women’s families did not have a net, and 8.7% of these tested positive compared to 4.9% of women whose family owned an ITN. For those who did not sleep under an ITN the previous night, 8.1% tested positive compared with 4.8% who slept under an ITN. Malaria prevalence by parity ranged from 5.5% (parity 0-1), to 5.4% (parity 2-3), and 6.5% (parity 4 or more). The two districts that bordered highly endemic countries had MIP prevalence rates of 10% and above. Those testing positive were treated according to national guidelines.
Despite a significant decline of 86% in malaria prevalence in the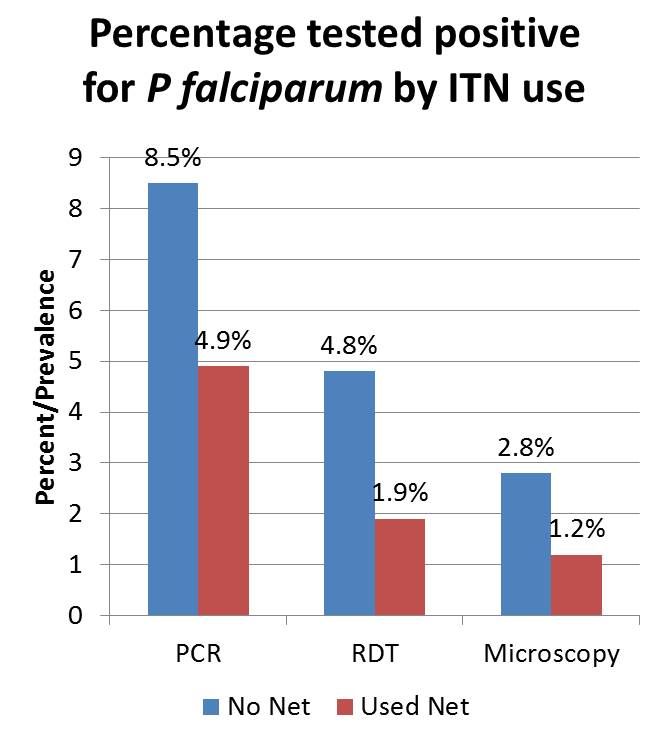 general population from 2005 to 2011, MIP prevalence remains high, especially in border districts. Our study also showed that ITN ownership and use among these pregnant women is below the national target. In order to address this gap, ITN distribution to achieve universal access, and educational campaign targeted at pregnant women on the use of ITN are recommended. Furthermore, early detection and treatment of MIP at ANC and regional collaboration to reduce cross-border malaria transmission should be prioritized.
general population from 2005 to 2011, MIP prevalence remains high, especially in border districts. Our study also showed that ITN ownership and use among these pregnant women is below the national target. In order to address this gap, ITN distribution to achieve universal access, and educational campaign targeted at pregnant women on the use of ITN are recommended. Furthermore, early detection and treatment of MIP at ANC and regional collaboration to reduce cross-border malaria transmission should be prioritized.
————————–
[1] Corine Karema, William R. Brieger, Irenee Umulisa, Aline Uwimana, Jeremie Zoungrana, Beata Mukarugwiro, Rachel Favero, Elaine Roman, Barbara Rawlins, Tharcisse Munyaneza, Fidele Ngabo, David Sullivan, Jean Baptiste Mazarati, Rukundo Alphonse, Agnes Binagwaho
Elimination &IPTp &ITNs Bill Brieger | 25 Oct 2015
Jhpiego Malaria Activities Featured in Posters at ASTMH Annual Meeting
 Today marks the start of the 64th annual meeting of the American Society of Tropical Medicine and Hygiene from 25-29 October 2015 in Philadelphia. Please stop by the poster sessions Monday, Tuesday and Wednesday to see a sampling of Jhpiego’s malaria programs. We are featuring Angola, Nigeria, Burkina Faso, Tanzania, Kenya and Rwanda. You can also discuss with Jhpiego staff at Booth #100 in the Exhibition Hall.
Today marks the start of the 64th annual meeting of the American Society of Tropical Medicine and Hygiene from 25-29 October 2015 in Philadelphia. Please stop by the poster sessions Monday, Tuesday and Wednesday to see a sampling of Jhpiego’s malaria programs. We are featuring Angola, Nigeria, Burkina Faso, Tanzania, Kenya and Rwanda. You can also discuss with Jhpiego staff at Booth #100 in the Exhibition Hall.
Poster Session A Monday 26 October 2015![]()
- LB-5094 – Readiness for Malaria Elimination: Using HMIS data to Map Malaria Test Positivity in Huambo Province, Angola – João Carlos F. Juliana1, William R. Brieger2, Jhony Juarez3, Connie Lee3, Clementino Sacanombo1 – 1Ministry of Health, Huambo, Angola, 2The Johns Hopkins University, Baltimore, MD, United States, 3Jhpiego, The Johns Hopkins University, Baltimore, MD, United States.
- 385 – Health Systems Strengthening: Improving quality of services for prevention of malaria in pregnancy through the Standards-Based Management and Reward approach in Kenya – Augustine M. Ngindu1, Gathari Ndirangu2, Sanyu N. Kigondu2, Isaac M. Malonza3 – 1USAID-MCSP, Kisumu, Kenya, 2USAID-MCSP, Nairobi, Kenya, 3Jhpiego Kenya, Nairobi, Kenya
Poster Session B Tuesday 27 October 2015
- 969 – Improving provision of malaria services through provider training in Burkina Faso – Ousman Badolo1, Stanislas Nebie1, Moumouni Bonkoungou1, Mathurin Dodo1, Thierry Ouedraogo1, Rachel Waxman1, William R. Brieger2 – 1Jhpiego, Baltimore, MD, United States, 2Johns Hopkins University, Baltimore, MD, United States
- 680 – Institutionalization of Quality of Care in Health Facilities Improves Management of Malaria in Pregnancy in Tanzania – Jasmine W. Chadewa, Rita Mutayoba – Jhpiego, Dar es Salaam, Tanzania, United Republic of Tanzania
- LB-5224 – Health systems strengthening – Advocacy facilitates availability of sulfadoxine pyrimethamine for prevention of malaria in pregnancy in Kenya – Augustine M. Ngindu1, Gathari G. Ndirangu2, Wekesa Kubasu3, Isaac M. Malonza4 – 1USAID-MCSP, Kisumu, Kenya, 2USAID-MCSP, Nairobi, Kenya, 3MOH, Bungoma, Kenya, 4Jhpiego,, Nairobi, Kenya Poster
- LB-5246 – Winning the fight against malaria in Huambo Province, Angola – João Carlos F. Juliana1, Jhony Juarez2, Clementino Sacanombo1, William R. Brieger3 – 1Ministry of Health, Huambo, Angola, 2Jhpiego, The Johns Hopkins University, Baltimore, MD, United States, 3The Johns Hopkins University, Baltimore, MD, United States
Symposium #83 Organized by Jhpiego, RBM Malaria in Pregnancy Working Group – Prioritizing Malaria in Pregnancy as Malaria Transmission Declines – Tuesday, October 27, 2015 1:45 – 3:30 PM
Poster Session C Wednesday 28 October 2015
- 1655 – Intermittent Preventive Treatment in Pregnancy: Increasing the Doses in Burkina Faso – Ousman Badolo1, Stanislas P. Nebie1, Mathurin Dodo1, Thierry Ouedraogo1, Rachel Waxman1, William R. Brieger2 – 1Jhpiego, Baltimore, MD, United States, 2Johns Hopkins University, Baltimore, MD, United States
- 1330 – Use of community health volunteers to increase coverage for integrated community case management in Bondo, Kenya – Savitha Subramanian1, Mark Kabue2, Dyness Kasungami1, Makeba Shiroya-Wadambwa3, Dan James Otieno4, Charles Waka3 – 1John Snow, Inc., Rosslyn, VA, United States, 2Jhpiego, Baltimore, MD, United States, 3Jhpiego, Nairobi, Kenya, 4John Snow, Inc., Nairobi, Kenya
- 1657 – LLIN distribution campaign processes: Lessons learned and challenges from Akwa Ibom State, Nigeria – John Orok1, Bright Orji2, Enobong Ndekhedehe2, William R. Brieger3 – 1Ministry of Health, Akwa Ibom State, Uyo, Nigeria, 2Jhpiego, Baltimore, MD, United States, 3Johns Hopkins University, Baltimore, MD, United States
- 1656 – Use of Long Lasting Insecticide-Treated Bednets in Akwa Ibom State Nigeria after a Major Distribution Campaign – Enobong U. Ndekhedehe1, John Orok2, Bright C. Orji1, William R. Brieger3 – 1Jhpiego, Baltimore, MD, United States, 2Ministry of Health, Akwa Ibom State, Nigeria, Uyo, Nigeria, 3Johns Hopkins University, Baltimore, MD, United States
Elimination &Eradication Bill Brieger | 24 Oct 2015
Eradication, Elimination: What is Feasible – WHO Global Malaria Program
Over the past few months several key malaria partners have been discussing the potentials for malaria elimination and mentioning target dates. Based on these discussions and publications Dr Pedro Alonso, Director, Global Malaria Programme or the World Health Organization has provided a reminder of WHO’s position and strategy. We share his comments for our readers below.
24 October 2015
Dear colleagues and partners,
 In recent weeks, you may have seen press articles stating that the United Nations and partners are calling on the world to eradicate malaria by the year 2040.
In recent weeks, you may have seen press articles stating that the United Nations and partners are calling on the world to eradicate malaria by the year 2040.
The World Health Organization (WHO) shares the vision of a malaria-free world and – to that end – we welcome the commitment of all of our partners. However, I would like to clarify the strategy, targets and timeline that our organization has endorsed at this point in time.
WHO’s work on malaria is guided, as you will recall, by the Global Technical Strategy for Malaria Elimination 2016-2030, adopted in May 2015 by the World Health Assembly. The strategy calls for accelerated action toward malaria elimination in countries and regions but does not set a time frame for global eradication.
This WHO strategy is complemented by the Roll Back Malaria advocacy plan, Action and Investment to Defeat Malaria 2016-2030. Both documents were the result of an extensive consultative process involving the participation of more than 400 malaria experts from 70 countries. They set ambitious but achievable global targets, including:
- Reducing malaria case incidence by at least 90% by 2030
- Reducing malaria mortality rates by at least 90% by 2030
- Eliminating malaria in at least 35 countries by 2030
- Preventing a resurgence of malaria in all countries that are malaria-free
The timeline of 2016-2030 is aligned with the 2030 Agenda for Sustainable Development, the new global development framework adopted by all UN Member States in September.
New WHO estimates
Recent news articles have reported a wide range of estimates on case incidence, mortality and global investment for malaria, which may have caused confusion. Please find below two documents with the latest WHO-approved estimates:
- A fact sheet with key global and regional estimates from the WHO-UNICEF report “Achieving the malaria MDG target,” published on 17 Sept. 2015. http://www.who.int/mediacentre/factsheets/fs094/en/ (see some excerpts below)
- An updated WHO general fact sheet on malaria.
http://www.who.int/malaria/media/malaria-mdg-target/en/
Best regards,
Dr Pedro Alonso
Director, Global Malaria Programme
World Health Organization
Elimination
Malaria elimination is defined as interrupting local mosquito-borne malaria transmission in a defined geographical area, typically countries; i.e. zero incidence of locally contracted cases. Malaria eradication is defined as the permanent reduction to zero of the worldwide incidence of malaria infection caused by a specific agent; i.e. applies to a particular malaria parasite species.
On the basis of reported cases for 2013, 55 countries are on track to reduce their malaria case incidence rates by 75%, in line with World Health Assembly targets for 2015. Large-scale use of WHO-recommended strategies, currently available tools, strong national commitments, and coordinated efforts with partners, will enable more countries – particularly those where malaria transmission is low and unstable – to reduce their disease burden and progress towards elimination.
In recent years, 4 countries have been certified by the WHO Director-General as having eliminated malaria: United Arab Emirates (2007), Morocco (2010), Turkmenistan (2010), and Armenia (2011). In 2014, 13 countries reported 0 cases of malaria within their own borders. Another 6 countries reported fewer than 10 cases of malaria.
The WHO Global Technical Strategy for Malaria 2016-2030 sets ambitious but achievable global targets, including:
- Reducing malaria case incidence by at least 90% by 2030.
- Reducing malaria mortality rates by at least 90% by 2030.
- Eliminating malaria in at least 35 countries by 2030.
- Preventing a resurgence of malaria in all countries that are malaria-free.