Community &Monitoring &Treatment Bill Brieger | 12 Nov 2013
Community registers in Akwa Ibom State, Nigeria track malaria treatment and integrated services
Below is the abstract for a poster being presented by a team from Jhpiego at the upcoming 62nd annual meeting of the American Society for Tropical Medicine and Hygiene November 13-17 2013 at the Marriott Wardman Park in Washington DC. If you are at the conference, stop by poster number LB-2289 on Friday and discuss with Bright Orji.

Community Directed Distributors bring their registers to the nearby clinic for monthly supervision meetings
Community Directed Treated with Ivermectin (CDTI) for onchocerciasis successfully reached 100,000 African villages with locally selected volunteers known as Community Directed Distributors (CDDs). Recognizing CDTI’s potential other health programs added a variety of interventions to the work of CDDs. Jhpiego (an Affiliate of Johns Hopkins University) successfully engaged communities and their CDDs in Akwa Ibom State, Nigeria to control malaria in pregnancy from 2007-11, and subsequently found the communities willing to expand into integrated community case management (ICCM) of malaria, diarrhoea and pneumonia. This report documents iCCM services given by CDDs.
The project mobilized 108 kin groups (100 +/- people) in 6 clinic catchment areas two Local Government Areas of the State. Each kin group selected 1-2 CDDs. Overall, 152 CDDs were trained by staff of local health centers. CDDs continued to provide intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine and then added malaria rapid diagnostic tests (RDTs); Artemisinin-based Combination Therapy for positive RDT results; oral rehydration solution and zinc tablets for diarrhea, and cotrimoxazole for pneumonia.
Data were extracted one year’s information from a sample of 68 community registers by three health staff using a checklist. During the period 2,202 clients were seen by CDDs with ages ranging from infancy to adulthood. Overall 33.3% were treated for malaria, 20.3% for pneumonia and 7.8% for diarrhoea (a few had multiple problems). Among the client visits, 30.6% were for pregnant women receiving a dose of IPTp.
RDTs were used with 1550 clients (70.4%) who had suspected malaria and 44.1% were positive. The breakdown of the 734 treated for malaria was positive RDT (93.1%), negative RDT (2.2%) and no test (5.2%). Community registers have shown that volunteer CDDs can provide a variety of front line health services, and can fairly correctly follow malaria testing and treatment procedures.
Advocacy &Communication Bill Brieger | 11 Nov 2013
Malawi Vice President Launches the 2013 SADC Malaria Day
Daniso Mbewe, the Knowledge and Information Management Officer of SARN has shared with us a Press Release from the Southern African Regional Network Secretariat (SARN) of the RBM Partnership in Southern Africa. The commemoration was held under the THEME: “Be free of Malaria in SADC Region”
 SALIMA, MALAWI, 08 November, 2013: The Vice President of Malawi, Rt. Hon. Khumbo Hastings Kachali, launched the 2013 SADC Malaria Day Events in the malaria endemic Lake Malawi town of Salima. The events were attended by Health Ministers and senior health officers and national malaria managers from SADC countries (Angola, Botswana, Lesotho, Malawi, Mozambique, Namibia, Tanzania Mainland and Zanzibar, Zambia and Zimbabwe, SADC Secretariat, SARN Secretariat, USAID, the uniformed Forces (military/police), RBM partners, provincial, district and local political, religious and traditional leaders, communities and school children.
SALIMA, MALAWI, 08 November, 2013: The Vice President of Malawi, Rt. Hon. Khumbo Hastings Kachali, launched the 2013 SADC Malaria Day Events in the malaria endemic Lake Malawi town of Salima. The events were attended by Health Ministers and senior health officers and national malaria managers from SADC countries (Angola, Botswana, Lesotho, Malawi, Mozambique, Namibia, Tanzania Mainland and Zanzibar, Zambia and Zimbabwe, SADC Secretariat, SARN Secretariat, USAID, the uniformed Forces (military/police), RBM partners, provincial, district and local political, religious and traditional leaders, communities and school children.
The presence of traditional dance troops, dreamers, actors (drama troops) and school children made the event colorful and highly entertaining. Of special mention is Illovo Sugar a member of the SARN private sector constituency which donated 1 million Malawi Kwacha for the event and provided a demonstration of the T3, IRS, LLINs, IPTP and BCC/IEC.
Senior Chief Kalonga thanked SADC and the Malawi government for bringing the event to his region because Salima has a lot of malaria which is impacting on development especially workers, school children, pregnant women, teachers and fishermen. He thanked the National Malaria Control Program for distributing LLINs and other interventions which are on-going in his region.
Malawi Minister, Hon. Catherine Gotani Hara – emphasized the need to continue protecting the women and that they should attend ANCs and demand for malaria protection while encouraging all members of the family and community to report early for treatment. She thanked the RBM and partners for the continued support and technical guidance from the WHO.
The Rt. Hon Khumbo Hastings Kachali, the Vice President of the Republic of Malawi, a former Minister of Health said that he was informed that there is now a trend showing a decrease in cases and deaths in Salima and he would like to see this replicated nationally. He however, warned the communities that this could be derailed by those people who use nets for fishing (Salima is a fishing community), sell nets, do not sleep under nets, do not complete thei r treatment and women who refuse to take IPTp. By 2015 he said “Malawi should have distributed over 10 million LLINs” much to the applaud of the participants.
r treatment and women who refuse to take IPTp. By 2015 he said “Malawi should have distributed over 10 million LLINs” much to the applaud of the participants.
The Vice President thanked SADC Member States and all those who attended and that this level of collaboration, interaction and information sharing should continue to blossom. He further emphasized that the attainment of the MDGs is a priority for all SADC countries and as the SADC chair, Malawi will continue to encourage countries and also to appraise the Heads of States on progress made and challenges the Ministries of Health are facing especially domestic funding, health infrastructure, equipment, shortage of human resources and skill levels.
The main outcome was high and community levels advocacy, SARN-RBM visibility, regional collaboration and community education via several drama/plays with malaria themes and messages.
Coordination &Monitoring Bill Brieger | 11 Nov 2013
Challenges in Malaria Health Information Collection and Coordination
Today This Day Live News reported on challenges of data coordination in the health system in Nigeria. Ndubuisi Francis reported that, “The multiplicity of conflicting data on health by various agencies is a major impediment to an effective and efficient health care delivery system in the country. Director, Disease Control and Immunisation, National Primary Health Care Development Agency (NPHCDA), Dr. Emmanuel Abanida, said resolving the conflict in the national health management information system (HMIS) is a step towards getting the system right.” The problem is not unique to Nigeria.

Health facility staff compile monthly data reports
To learn more about how this problem affects malaria data we discussed with two staff of the Jhpiego office in Abuja, Gbenga Ishola and Bright Orji, who have been involved for many years in malaria monitoring and evaluation activities at national, state and local levels. The results of this discussion follow:
1. Incorporating Community Health Worker Data into HMIS
As the country moved toward community case management to reach coverage targets, the HMIS has worked with NMCP to establish a community data collection template. However, the level of utilization of the community level register is poor. Also the integration of this into facility output remains a key challenge. Furthermore, there has not been a feedback mechanism to the community of data collected from them. So, it is not only collection of data but use of data for decision-making whether at the Local Government (LG) level, facility or community remains part of the challenge.
2. Movement of Data from Facility to District to State to National
There is an existing data flow pattern. Data from facility HMIS registers are expected to be collated on monthly basis into a monthly summary form at facility level. The summary forms are sent to the Local Government Monitoring and Evaluation Unit which then sends this to the state level. Data flow is also not as smooth as intended. Most often facilities do not collate and send to the LG, and thus state data reporting that is suppose to be quarterly is distorted. The obvious complaint is always logistics.
The National Malaria Control Program (NMCP) monitors state data reporting by aggregating total number of facilities reporting each month and determining reporting rate for the states. Each state reports total number of health facilities in the state, and how many of these facilities submitted a monthly report during review period. For example, if a state has 1,000 health facilities but only 500 submitted monthly reports, the state would have scored 50% in data reporting. This is to encourage state to improve on data collection and reporting and is part of the report and discussions at the annual malaria program’s manager meetings.
3. Parallel Reporting Systems
There are two examples of parallel systems through which malaria data move. The National Primary Health Care Development Agency, a section of the Ministry of Health responsible for assisting LGs strengthen their primary care systems collects health data from those facilities in addition to the facilities reporting through the HMIS. Recently the Director of the HMIS indicated that his unit is trying to harmonize the existing system. The completeness of each system varies depending on how LGs and states decide to report.
 Since the HMIS collects only a limited selection of malaria indicators, the NMCP makes an effort to collect more detailed statistics of all services. Some of the indicators monitored by NMCP are not in HMIS. The consequence is that health workers often abandon the NMCP register because it contains more entries than HMIS.
Since the HMIS collects only a limited selection of malaria indicators, the NMCP makes an effort to collect more detailed statistics of all services. Some of the indicators monitored by NMCP are not in HMIS. The consequence is that health workers often abandon the NMCP register because it contains more entries than HMIS.
The HMIS collects 1) Long-lasting insecticide-treated nets (LLINs) provided and 2) doses of Intermittent Preventive Treatment (IPTp) given (1st and 2nd). NMCP additionally tracks number of fever cases, Rapid Diagnostic Tests (RDTs) conducted (and whether RDT results are negative, positive or invalid), and antimalarial medicines administered (whether quinine or ACT).
While the National HMIS unit is working to harmonize the data collection formats for all diseases including malaria cases, bringing the NMCP to participate in meetings and discussions has been a major problem. This makes it very difficult for the HMIS to be able to quote data relating to specific diseases when necessary.
4. Special Data Requirements
As in other countries, the Global Fund expects countries to report of a regular, quarterly basis on achievements based on their currently operating grant. The data required for these reports is essential for maintaining the flow of funding, but this information is not necessarily within the basic HMIS set of indicators. Global Fund is interested in consumption data for forecasting for national needs, but this has been very difficult to collect due to some of the above challenges.
Bright Orji and Gbenga Ishola review malaria in pregnancy data with local government nurse-midwife
The number and detail of indicators reported to the Global Fund for Nigeria’s Round 8 malaria grant reflect the complexity of reporting required that would not be included in HMIS. Below are a few examples of the malaria treatment related indicators only. HMIS would not be collecting program process data like training and does not really reach the private sector.
- Number of children under five with uncomplicated malaria receiving ACT treatment according to National guidelines (all oints of care)
- Number of children under five with uncomplicated malaria receiving ACT treatment according to National guidelines through the public sector
- Number of people (over 5) with uncomplicated malaria receiving ACT treatment according to National guidelines through the public sector
- Number of person (over 5) with uncomplicated malaria receiving ACT treatment according to National guidelines through the private sector
- Percentage of participating health facilities in the public sector reporting no stock out of ACTs for 1 week or more within the last 3 months
- Number of health care providers trained in malaria case management and prevention
- Number of CSO members trained on case mangement and prevention of malaria
- Number of Health care providers trained on pharmacovigilance
In order eventually to eliminate malaria detailed monitoring and surveillance data are needed in real time. Coordinating these data needs with a routine national HMIS will always be challenging because disease elimination is anything but a routine process.
IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2013
Ghana: Progress on IPTp, but not yet sustained high coverage
The 2011 Multiple Indicator Cluster Survey (MICS) from Ghana demonstrates the challenges we have in moving along the pathway toward malaria elimination. People will recall that the Roll Back Malaria indicators were for endemic countries achieve 80% coverage on basic malaria interventions by 2010 and sustain these to achieve Millennium Development goals by 2015 and then move on to pre-elimination of the disease where less than 1/1000 people at risk in a country actually experienced malaria. Now of course, everyone is talking about universal coverage of basic services, not just 80%.
The 2011 Ghana MICS reports on the standard RBM indicator of two doses of intermittent preventive treatment (IPTp) with sulphadoxine-pyrimethamine (SP) during antenatal care (ANC), although Ghana has for some time aimed at three doses. Also current WHO guidance for IPTp recommends IPTp in stable endemic countries at one dose for every antenatal care visit after quickening, which could mean three or four times. So the 2011 MICS shows 83% of recently pregnant women surveyed got one dose of IPTp during ANC while only 65% received two.
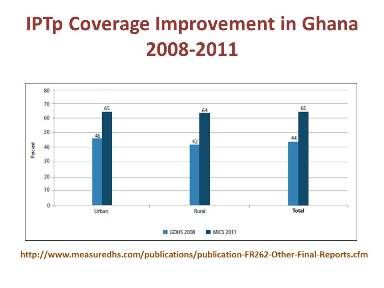 The chart to the right does show progress in IPTp coverage between the 2008 Demographic and Health Survey and the 2011 MICS. a jump from 44% to 65% for the two doses, and progress should be acknowledged, but as pointed out at the recent Pan Africa Malaria Conference in Durban, we must not work around the edges to eliminate malaria, but tackle the higher prevalence countries and areas directly and ensure that malaria is truly eliminated.
The chart to the right does show progress in IPTp coverage between the 2008 Demographic and Health Survey and the 2011 MICS. a jump from 44% to 65% for the two doses, and progress should be acknowledged, but as pointed out at the recent Pan Africa Malaria Conference in Durban, we must not work around the edges to eliminate malaria, but tackle the higher prevalence countries and areas directly and ensure that malaria is truly eliminated.
Why are coverage figures low – and this is not just a problem in Ghana? At least 96% of pregnant wom en in Ghana attend ANC with a skilled provider: 95% make two ANC visits, 89% make three and 86% are reported to make four. What we may be seeing are missed opportunities.
en in Ghana attend ANC with a skilled provider: 95% make two ANC visits, 89% make three and 86% are reported to make four. What we may be seeing are missed opportunities.
Are gaps due to health worker errors, SP stock-outs or client refusals? This needs to be investigated and rectified.
Ideally pregnant women should also get an insecticide treated net on their first ANC visit regardless of distribution through mass campaigns. Unfortunately the MICS 2011 shows that only 32% of pregnant women overall had slept under a treated net the previous night, and even in households with nets, only 58% had slept under them. Clearly malaria in pregnancy control and scale-up needs higher priority in Ghana as well as the rest of Africa.
Community &ITNs Bill Brieger | 06 Nov 2013
Building Community Capacity in Malaria Control: the Malaria Communities Program
The Malaria Communities Program (MCP) was launched on December 14, 2006. Through 20 awards to 18 partners in 12 countries, the President’s Malaria Initiative (PMI) has supported efforts of communities and nongovernmental organizations (NGOs) to combat malaria at the local level. Excerpts from one of the MCP case studies are found below.
This case study examines different models of community outreach and engagement implemented by five MCP partners: the Christian Reformed World Relief Committee (CRWRC) Malawi, HealthPartners Uganda, Catholic Medical Mission Board (CMMB) Zambia, Aga Khan Foundation (AKF) Mozambique in partnership with Progresso, and Lutheran World Relief (LWR) Mali. MCHIP collected multiple forms of data from these five partners using qualitative methods, including individual interviews with key project personnel and review of key documents.
MCHIP then compared data across projects to better understand the overall contributions made by MCP. Some partners conducted surveys, and this report includes relevant quantitative data. Data are limited by a lack of standardized reporting on this topic. Future studies about the relationship between community capacity and malaria control could utilize frameworks described in relevant literature for planning and reporting results.
 The major sub-theme emerging from the data was effective utilization of community volunteers as a way to build community capacity and sustain project results. Each partner’s strategy to engage and retain volunteers included these key attributes: selection of volunteers, motivation/retention of volunteers, ensuring sustainability of the volunteer program, and addressing challenges. Building community capacity can be described as the means by which communities and individuals enhance their skills, abilities, resources, and commitments to identify challenges and solutions in their communities, and nurture their unique talents and leadership. In this process, individuals and groups increase their abilities to impact the health and vitality of their communities.
The major sub-theme emerging from the data was effective utilization of community volunteers as a way to build community capacity and sustain project results. Each partner’s strategy to engage and retain volunteers included these key attributes: selection of volunteers, motivation/retention of volunteers, ensuring sustainability of the volunteer program, and addressing challenges. Building community capacity can be described as the means by which communities and individuals enhance their skills, abilities, resources, and commitments to identify challenges and solutions in their communities, and nurture their unique talents and leadership. In this process, individuals and groups increase their abilities to impact the health and vitality of their communities.
MCP partners trained, empowered, and equipped volunteers with skills and tools to promote key messages about malaria prevention and treatment. MCP partnerships with National Malaria Control Programs (NMCPs) and community members have strengthened local ownership by facilitating community-driven processes for volunteer selection and supervision.
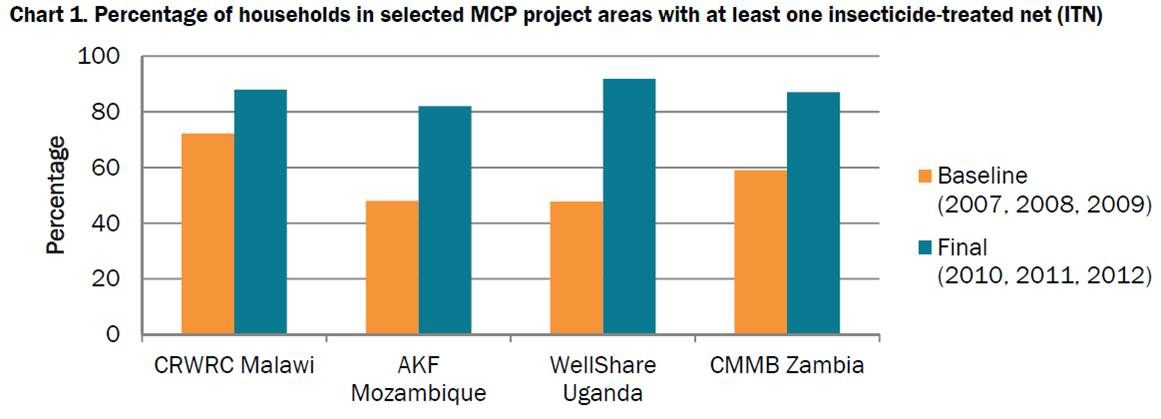
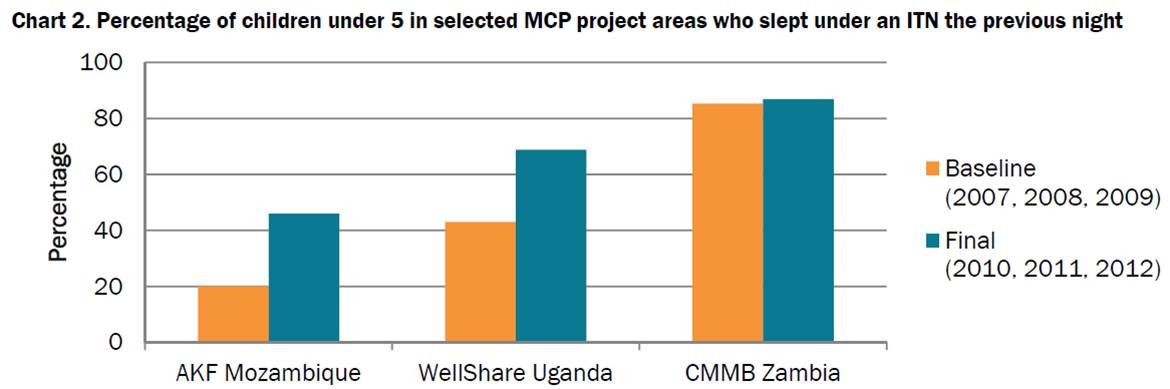 Trained volunteers have helped increase community demand for nets and fostered trust between health workers and community volunteers, creating a foundation for communities to control malaria. Charts 1 and 2 show positive trends in selected MCP project areas in net ownership and use, which may result from strengthened community capacity, as seen in the Zambia study.
Trained volunteers have helped increase community demand for nets and fostered trust between health workers and community volunteers, creating a foundation for communities to control malaria. Charts 1 and 2 show positive trends in selected MCP project areas in net ownership and use, which may result from strengthened community capacity, as seen in the Zambia study.
Download and read the full case study at: http://www.mchip.net/node/2069
See also: Underwood C et al. 2013 Community capacity as means to improved health practices and an end in itself: Evidence from a multi-stage study. Intl Quarterly of Community Health Education 33(2): 105–127.
Malaria in Pregnancy &Treatment Bill Brieger | 04 Nov 2013
Improving case management of malaria during pregnancy by antenatal care providers in Akwa Ibom State, Nigeria
Bright Orji, William Brieger, Emmanuel Otolorin and John Orok presented today at the 141st APHA Annual Meeting in Boston of Jhpiego’s  experiences with malaria in pregnancy in Akwa Ibom State Nigeria. A summary appears below.
experiences with malaria in pregnancy in Akwa Ibom State Nigeria. A summary appears below.
In Nigeria malaria causes approximately 11% of maternal deaths. Malaria is responsible for 63% of hospit al admissions and 70% of illness among pregnant women. While intermittent preventive treatment (IPTp) and Long Lasting Insect icide-treated Nets (LUNs) are supposed to be given to pregnant women to prevent the dis·ease, coverage is poor.
Unfortunately since malaria is often being treated presumptively, pregnant women st ill die from other fever-related illnesses. Use of rapid diagnostic test (RDTs) to confirm malaria before treatment provides an opportunity for earlier recognition of febrile illnesses not due to malaria.
This study assessed the pattern of malaria diagnosis and treatment in pregnant women attending Antenatal care (ANC) in Akwa Iborn State, Nigeria. Record cards of pregnant women attending six government owned ANC before and after staff training on malaria diagnosis using RDTs.
The patients’ cards were drawn from ANC clinics with first non- follow-up visit of the year before training (February 20 10) and after (March 20 11) by three nurses/midwives.
Health care providers fever gave 85% of 3 13 women attending ANC antimalarial drugs before the introduction of RDTs training. Afterwards 82% of 179 febrile women were tested with RDTs. All 29 with positive RDT received artemisinin-based combination therapy, 6 RDT-negative women got ACTs, and no women who were not tested were treated for malaria.
Training encouraged health workers to adherence rational prescribing of antimalarials and made it possible t o offer better management of other fever-related illnesses during pregnancy. Support is now needed to scale-up RDTs use in ANC clinics in Nigeria.
Uncategorized Bill Brieger | 04 Nov 2013
Working together towards success in controlling malaria in Huambo Province, Angola
The following colleagues from the Ministry of Health in Huambo Angola and Jhpiego presented their work at the 141st American Public health Annual Meeting in Boston yesterday: Frederico Juliana, Jhony Juarez, Amandio Natito, and Lelo Zola. Please see their contribution below.
 Malaria is the first cause of morbidity and mortality in Angola. Angola has 18 provinces and an estimated population around 17 million. There are three epidemiologic classes: hyper-endemic (Northern part of the country), stable meso-endemic area (Central) and unstable meso-endemic area (South).
Malaria is the first cause of morbidity and mortality in Angola. Angola has 18 provinces and an estimated population around 17 million. There are three epidemiologic classes: hyper-endemic (Northern part of the country), stable meso-endemic area (Central) and unstable meso-endemic area (South).
In the last ten years, the Ministry of Health, the National Malaria Control Program, and national and international organizations have made efforts to control it. In Huambo Province, where about 14% of the total Angolan population lives, the number of malaria cases decreased by 85% and the deaths decreased by 98% to just 31 deaths between 2008 and 2012.
 Factors that have contributed to the reduction of malaria cases include increase in number of health professionals, principally doctors, work with organized communities, health fairs (Uhayele Vimbo) for rural/ isolated populations. In addition major malaria interventions such as rapid malaria tests and microscopes, combined antimalarials, spraying, ITN distribution, improvement in diagnosis and treatment, equipment for spraying, anti-larva projects were deployed more widely.
Factors that have contributed to the reduction of malaria cases include increase in number of health professionals, principally doctors, work with organized communities, health fairs (Uhayele Vimbo) for rural/ isolated populations. In addition major malaria interventions such as rapid malaria tests and microscopes, combined antimalarials, spraying, ITN distribution, improvement in diagnosis and treatment, equipment for spraying, anti-larva projects were deployed more widely.
Reaching all municipalities, communes and neighborhoods with these services and population-level health education campaigns, improvements in the health information system and a rapid alert, earlier care-seeking for malaria symptoms led to lives saved. Number of malaria cases and deaths in Huambo decreased between 2008 2012 from 620,300 to 87,852 and from 1,559 to 31 respectively.